Nearly 100 billionaires and their spouses have donated to reelect Susan Collins

Republican U.S. Sen. Susan Collins announced her reelection campaign in February by posting a video that showed her opening a box of New Balance running shoes.
“This is perfect for 2026,” she said to the camera as she held up a sneaker. “Because I’m running.”
The video didn’t mention that New Balance’s owner and chairman, billionaire Jim Davis, gave $1 million to the super PAC supporting Collins’ campaign seven months prior. The company is based in Boston and has manufacturing facilities in Maine. It was one of four donations Davis made last year to the network of committees raising money for Collins.
Davis, who is worth an estimated $6.1 billion, is one of at least 79 billionaires who donated to Collins’ network between January 2025 and May 20, 2026, according to a Maine Monitor analysis of Federal Election Commission campaign finance data. If billionaires’ spouses are included in the tally, the number rises to 97.
Collectively, the group of nearly 100 billionaires and spouses has donated $9.8 million to the Collins network since the start of 2025, representing a third of what groups supporting Collins raised from all donors.
The total from billionaires stands in stark contrast with the fundraising of her opponent, Democrat Graham Platner, whose campaign has mostly attracted smaller amounts of funds but from many more people. Platner, who won his party’s primary election Tuesday, has received at least $24,000 from five billionaires, a fraction of 1 percent of his total haul.
The breadth of billionaire funding for Collins shows how the race, which could decide control of the U.S. Senate, has drawn national interest and funding from some of the wealthiest people in the world, a group that has made up a growing share of election spending in recent years. Billionaires accounted for 19 percent of all federal election contributions in 2024, up from just 0.3 percent in 2004, according to a New York Times analysis from earlier this year.
Billionaires and their spouses gave $529,000 to the Collins campaign directly; $370,000 to the Collins Victory Committee, a joint fundraising committee that has disbursed funds to the other committees; $100,000 to Dirigo PAC, the leadership committee Collins uses to raise money for other candidates; and $24,000 to Susan Collins for Maine, a joint fundraising committee. But the billionaires have mostly opted to send their donations, nearly $9 million, to Pine Tree Results PAC, a super PAC dedicated to electing Collins that, unlike the others, is not subject to contribution limits.
Pine Tree Results PAC has financed attack ads against Platner since April and has booked $24 million in ads leading up to the general election in November, according to data from AdImpact.
The network of five groups supporting Collins is linked through a series of joint fundraising agreements, which are legal arrangements that allow them to raise money together and then disburse the funds according to a predetermined formula. For the first time in Collins’ career, a super PAC — Pine Tree Results — is linked to her fundraising apparatus through those agreements, an arrangement made possible thanks to a 2024 advisory Federal Election Commission opinion. The super PAC also shares a treasurer with the Collins Victory Committee and Dirigo PAC.
Counting all her donations, including both from billionaires and others, the Collins network has raised about $30 million since the beginning of last year, with $12 million going to her campaign.
The Platner campaign, meanwhile, raised $16.3 million over that time. The total does not include the $200,000 his campaign said it raised in the 24 hours after The New York Times published a story last week detailing what it described as Platner’s “unsettling” behavior with three former girlfriends. The Platner campaign has no joint fundraising agreements with any other committees, according to federal campaign finance filings, and no super PAC dedicated to supporting his candidacy. (Platner has said that super PACs “should be outlawed.”) Experts speculated, however, that big outside money will likely move toward Platner now that he has clinched the Democratic nomination.
The Monitor counted billionaire donors by comparing the names on the Forbes 2026 World’s Billionaire List to Federal Election Commission donor information, which included reviewing location and occupation information to eliminate the possibility of erroneous matches based on similar names.
The Collins campaign did not respond to a request from The Monitor for an interview with the senator and then declined to answer questions over email.
The amount billionaires gave in support of Collins is similar to the amount that small-dollar donors — those giving $200 or less — contributed to the Platner campaign. Billionaires gave $9.8 million in support of Collins, while small-dollar donors gave $9.6 million to support Platner. The Collins campaign raised about $980,000 from small-dollar donations.
“While Susan Collins’ campaign is backed by billionaire donors, our campaign is built on a movement funded by the people, with an average donation of $26,” wrote Ben Chin, Platner’s campaign manager, in an email.
The majority of the billionaire donations to Collins this cycle are from billionaires who made their money in alternative investments, including hedge funds and private equity. Ken Griffin, founder and CEO of Citadel LLC, donated $2.5 million to the Pine Tree Results Super PAC, the largest individual donation backing Collins since 2025. Stephen Schwarzman, the founder and CEO of Blackstone dubbed “the king of private equity,” donated $2 million. Schwarzman and the private equity industry were some of Collins’ biggest boosters in her last campaign in 2020.
Other billionaire Collins donors include Palantir co-founder Alex Karp; Melinda French-Gates, ex-wife of Microsoft founder Bill Gates; New England Patriots owner Robert Kraft; and Elizabeth Uihlein, husband of Richard Uihlein, the main financial backer of the effort to place a referendum question about trans athletes on Maine’s ballot this year.
The billionaire donors supporting Collins have a net worth of $888 billion, or nearly nine times Maine’s entire economic output in 2025. None are Maine residents.

The Platner campaign received donations from at least five billionaires. It received $1,500 from Jennifer Pritzker, a cousin to fellow billionaire and Illinois Gov. J.B. Pritzker; a total of $12,000 from Jon and Pat Stryker, heirs to the Stryker medical equipment empire; $3,500 from Christy Walton, who married into the Walton family; and $7,000 from Democratic megadonor and hedge fund founder George Soros. Together, they are worth an estimated $42.3 billion.
The difference between billionaire contributions to the two candidates is not surprising given Collins’ long Senate tenure, her position as chair of the powerful appropriations committee and Platner’s anti-billionaire message, said Mark Brewer, a political science professor at the University of Maine.
“We generally know that, in contemporary American politics, big money from wealthy donors generally tends to head in the direction of Republicans more than Democrats,” he said.
Meanwhile Democrats dating back to Howard Dean and Barack Obama have shown the possibility of raising huge sums from small-dollar donations, he added.
“It’s two different ways to get there, but you both get there,” Brewer said.
Just 3 percent of the total that Collins’ groups raised came from donors who gave $200 or less. In comparison, about 60 percent of donations to Platner’s campaign came from those smaller donations.
It’s not possible to track the state where smaller, “unitemized” donations came from. Committees are required, however, to provide the Federal Election Commission information about donors who contribute more than $200 across all federal campaigns, including their state of residence. These donations are called “itemized donations.” Both campaigns have relied heavily on out-of-state money for their itemized donations.
Of those larger donations to the Collins network, about 3 percent came from Maine.
Platner’s trackable donations were more likely to be from Maine: About 22 percent were from the state, according to the Federal Election Commission.
That’s actually a large percentage of in-state donations for a Senate campaign, said Nicholas Jacobs, a professor of American government at Colby College who has studied out-of-state donations in Senate campaigns. Maine contributed more itemized funding to Platner than any other state through May 20, according to the Federal Election Commission.
“That’s rare in general and exceptionally rare for a small state,” Jacobs said.
But now that Platner has won his primary, big money may start flowing his way. Jacobs predicted that Platner will likely get the backing of a super PAC at some point this summer.
“That’s just the way politics works,” Jacobs said.
In the wake of Citizens United
This is the first time that Collins has been running for reelection since the Federal Election Commission issued an advisory opinion that allowed super PACs to join joint fundraising efforts, and Collins has taken advantage of the change.
Before 2024, campaigns — which are subject to donor limits — could not be connected to super PACs, which are not subject to limits on donor contributions. Super PACs were created in the wake of the Citizens United Supreme Court decision, which ruled that groups independent of campaigns have a First Amendment right to raise and spend money supporting or attacking candidates without limits, so long as they aren’t coordinating with campaigns.
In 2024, the Federal Election Commission issued an advisory opinion allowing South Carolina Republican Sen. Lindsey Graham’s campaign to enter into a joint fundraising agreement with the super PAC supporting his candidacy. Commission members voted, 5-1, to permit the arrangement because Graham and his campaign told the commission they “will not discuss the nonpublic campaign plans, projects, activities, or needs of Senator Graham or his campaign with Super PAC,” according to the advisory opinion.
Critics, including the Democratic Party’s House and Senate fundraising arms, argued the arrangement was a clear violation of the ban on coordination, a ban that they argued has been regularly circumvented since the creation of the super PAC in 2010.
In her dissent, former Democratic Federal Election Commission member Ellen Weintraub wrote that “the Commission has already created far too many holes in what should be a solid wall dividing candidates and their committees from the super PACs that support them.” In 2025, Trump fired Weintraub from the commission shortly after she became chair and didn’t name a replacement. Shortly after that, the agency lost a quorum of commissioners, effectively sidelining it from its election watchdog duties since April 2025.
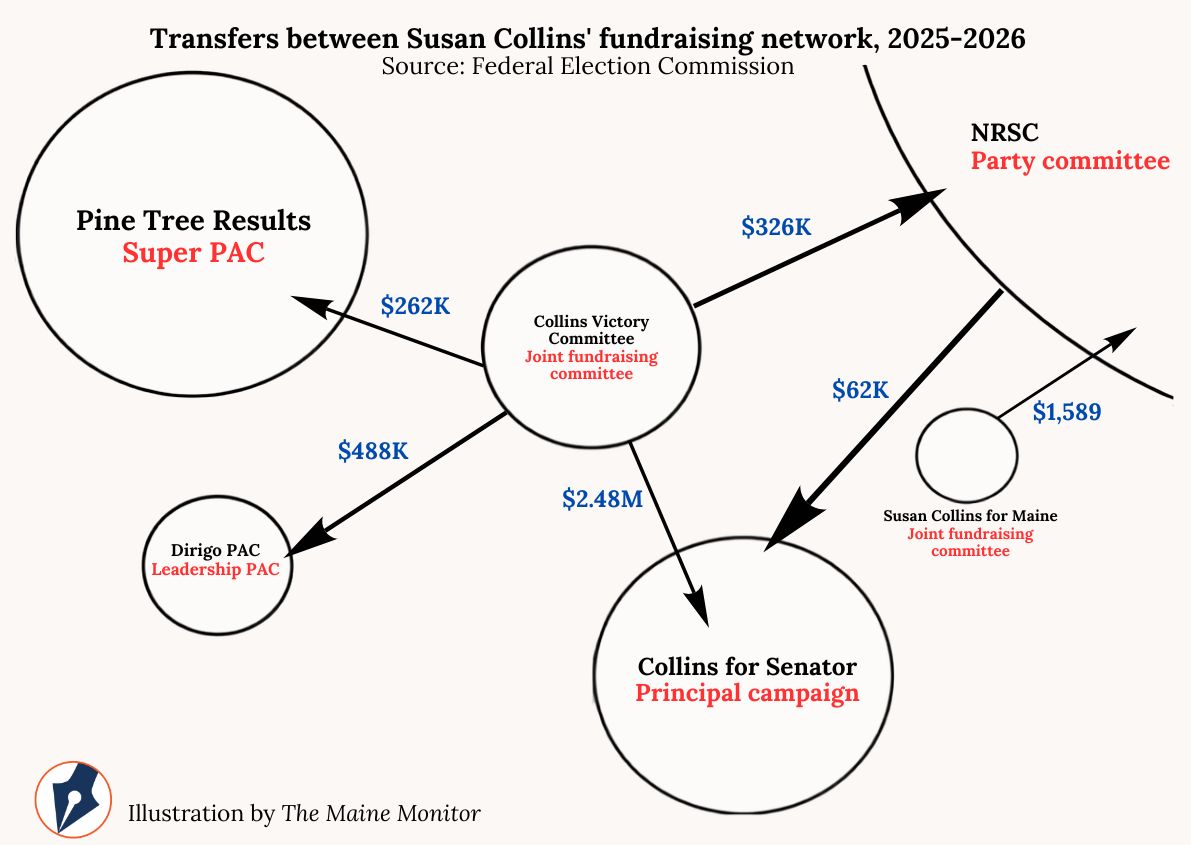
The 2024 advisory opinion opened the door for the Collins campaign to connect with the Pine Tree Results Super PAC. The campaign and the PAC each have a joint fundraising agreement with the Collins Victory Committee, which has transferred funds to both organizations. Most of this money, a total of $2.4 million, has gone to the Collins campaign.
The Pine Tree Results Super PAC and the Collins Victory Committee share a treasurer, and all three groups have paid the same fundraising and event planning consultant, the Morning Group, based in Washington, D.C., Federal Election Commission records show.
Other outside groups are also spending large amounts on the race. For example, the Senate Leadership Fund, which is the main fundraising vehicle for Senate Republicans, has raised $175 million since the start of 2025 and has booked $29 million in ads for the race pitting Collins against Platner.
Many of the donors to the Senate Leadership Fund also donated to parts of the Collins fundraising network, including Schwarzman and hedge fund manager Paul Singer. Other billionaires have donated large sums to the Senate Leadership Fund as well, including casino magnate Miriam Adelson, who donated $30 million, and Elon Musk, who gave $10 million.
On the other side of the aisle, Democratic super PAC WinSenate has booked $25 million in ads in Maine’s Senate race. WinSenate is funded by the Senate Majority PAC, the main fundraising vehicle for Senate Democrats. It has raised $115 million this cycle, and includes funds from billionaires such as Cable TV magnate Amos Hostetter Jr., who gave $2 million, and Netflix cofounder and chairman Reed Hastings, who contributed $1 million.
Both the Republican Senate Leadership Fund and the Democratic Senate Majority PAC are beneficiaries of large amounts of funds contributed by 501(c)4 nonprofits that aren’t required to reveal their donors. That type of funding has been dubbed “dark money” due to the lack of transparency about its sources.
This cycle, the Senate Leadership Fund has raised $46 million from conservative dark money group One Nation, while the liberal dark money group Majority Forward has donated $33 million to the Democratic Senate Majority Fund. It’s unclear how much of that money came from billionaires.
















