Georgia public health leader sounds alarm as report confirms spike in pregnancy-related deaths
Of the deaths studied in the new report, 113 were concluded to be related to pregnancy – and 89% of them were deemed preventable, meaning they had “at least some chance of being prevented,” according to the report.
The Current is an inclusive nonprofit, non-partisan news organization providing in-depth watchdog journalism for Savannah and Coastal Georgia’s communities.
Mountain State Spotlight explains: West Virginia’s opioid settlement foundation will soon have board members. Here’s how they’re picked
In the coming days, local government leaders across West Virginia are set to elect five board members for the foundation tasked with managing the majority of the state’s opioid settlement funds, a sum that totals right around $1 billion as of July. The new members of the West Virginia First Foundation will join Dr. Tom Kelly, an emergency medicine physician who was elected last week, and five members chosen by Gov. Jim Justice. The governor has also indicated that he’ll make his selections “really soon.”
Selecting the right people for these positions is essential, says Drema Hill, a West Virginia School of Osteopathic Medicine professor who helped the Attorney General’s Office determine how the state can spend its opioid settlement winnings.
“It is really going to have the power to make the decisions over these funds,” Hill said. “That’s why it’s very important who is elected to be on this board.”
We break down how West Virginia local governments are choosing their board members, how the foundation can spend its settlement funds, how well those members will represent areas most impacted by the substance use crisis and how transparent the foundation’s operations will be.
How are the opioid settlement foundation board members chosen for each region?
While West Virginia Attorney General Patrick Morrisey and other state lawyers were pursuing lawsuits against pharmaceutical supply chain companies, they developed a Memorandum of Understanding for the money from the lawsuits. The memorandum guides how the state can spend this money and established governing guidelines for the West Virginia First Foundation.
The document split the state into six regionsbased on existing designations from the state’s Bureau for Behavioral Health. Each region will have one resident serving as a board member for the foundation.
Officials from the towns, cities and counties of each region — with the exception of people from seven small local governments that never signed on to the memorandum — can nominate one person to be their region’s board member. Once all the nominations are in, the regions will host public meetings, where representatives from each local government included will vote on the candidates.
So far, the only meeting that’s taken place has been the one for Region Six, a series of southern West Virginia counties that were targeted by prescription drug distributors. Its local elected officials selected Kelly. The other five regions will choose their representatives on July 12 and July 13.
Who can be nominated?
The memorandum says board members should have expertise that could be helpful for guiding the foundation; examples range from substance use treatment practitioners to people experienced in finance.
A letter from Morrisey’s office to local governments says that nominating current elected officials is “highly discouraged.” According to his press secretary, that’s an attempt to prevent the selection from becoming political.
But that hasn’t stopped local governments from nominating elected officials. Mercer County Commissioner Greg Puckett was nominated for Region Six’s board seat but ultimately not selected.
In Region Three, an area made up of counties in the Mid-Ohio Valley, Parkersburg Mayor Tom Joyce will be on the ballot. Over the past two years, Joyce has, contrary to local data, attributed rises in Wood County crime to local substance use treatment efforts and successfully lobbied for state legislation that prevents Wood County from adding more treatment facilities. He did not respond to phone and email interview requests for this story.
Vienna Mayor Randall Rapp, who nominated the Parkersburg mayor for the board, cited Joyce’s professional experience working for hospitals as a major reason why he nominated him.
“I just think that [with] his background and his character, Tom will do the right thing,” Rapp said.
Wood County Commissioner Blair Couch was less comfortable with the prospect of Joyce as the Region Three representative. His commission nominated Westbrook Health Services president Kevin Trippett, and Couch said he would prefer someone like Kelly.
“I think politicians can be swayed more than a doctor from Raleigh County,” Couch said.
Will the foundation board be fair to the places most impacted by the crisis?
The money will be split according to a formula that assigns percentages — based on a municipality’s population, number of prescription pain pills received, and overdose death count — of how much of West Virginia’s total opioid crisis took place in an area.
For example, the formula determined that about 9% of the total crisis took place in Cabell County and Huntington. It calculated a similar estimate for Kanawha County and Charleston.
But each region will still only get one vote on the foundation. That means that despite the calculation that Region Five, which includes both Kanawha and Cabell counties, was affected more than other regions, it will have the same vote on the board as Couch’s Region Three.
“How can you have Cabell and Kanawha in the same region?” Couch asked. “Those two big ass counties, who have suffered a lot through the opioid [epidemic], are going to have one vote on this 11-member panel.”
How transparent will the foundation be?
Drema Hill says the West Virginia First Foundation is being set up as a private nonprofit to discourage the funds from being politicized and misused. But this has raised questions about whether the foundation will be subject to the same rules as government organizations.
Morrisey’s press secretary did not respond to phone and email questions asking whether the foundation will be subject to the state’s Freedom of Information Act. But courts have previously ruled that private foundations created by state authorities are subject to the law, according to Suzanne Weise, a West Virginia University law professor who specializes in government transparency.
A list of “frequently asked questions” developed by the Attorney General’s Office says that the foundation won’t be subject to the state’s Open Meetings Act. The memorandum does say that all meetings related to the foundation should be open to the public and gives the state’s attorney general the power to audit it. But some local government officials have already raised concerns about whether those provisions will create enough accountability for the organization.
How will the foundation spend the settlement money?
Once the attorneys’ fees for the settlements are finalized, the West Virginia First Foundation will be responsible for managing hundreds of millions of dollars. The board members are supposed to invest the majority of that sum, but the memorandum also instructs them to distribute 20% of the foundation’s yearly budget to the six regions each of the next seven years.
Each regional board member will also double as their area’s director; that job entails leading regional governing groups that decide how their shares of the money get spent. The foundation’s board members will collectively be responsible for determining the process by which West Virginia government and non-government organizations can apply for regional funds.
Conny Priddy, the program coordinator of Huntington’s Quick Response Team, is confident the money will help reduce the damage of the state’s opioid crisis. But she worries it won’t be enough.
In the 2021 trial that pitted Huntington and Cabell County against drug distribution companies, an epidemiologist and a forensic economist estimated that it would take $2.5 billion just to address the problem in that county. In the wake of U.S. District Judge David Faber’s ruling in favor of the drug distributors, lawyers for Huntington and Cabell have appealed the decision to the 4th U.S. Circuit.
Now, the foundation will only have access to a portion of $1 billion to address problems throughout the entire state. Priddy said some money is better than nothing, but she doesn’t know what impact it will ultimately have for the West Virginia families who have suffered the most.
“I hate to say it, but you can’t throw a little bit of money at it and then expect the problem to go away,” she said. “It has become generational.”
Disclaimer: Weise is the secretary of Mountain State Spotlight’s Board of Directors.
For Decades, the Top Rural Health Issue Has Been Access to Basic Care; Now It’s Mental Health and Addiction
For the first time in 20 years, mental health and addiction are more pressing health concerns than getting access to basic healthcare, according to a survey of rural stakeholders.
Rural Healthy People 2030, released by the Southwest Rural Health Resource Center, surveyed a national sample of people “working to improve the lives and health of rural Americans,” to determine the most important issues facing rural residents. Participants included people working in health care, public administration, education, human services, and other fields.
In 2010 and 2020, the biggest issue in the survey was access to health care.
While access to health care remained one of the top five issues according to survey respondents, researchers said, the growing impact of mental health and addiction took the number one and two spots on the list regardless of age, race, region or occupation.
“For the past two decades, health-care access has been, far and away, the most important topic no matter how we cut the data,” said Timothy Callaghan, one of the survey authors. “The fact that mental health and addiction came out ahead of health-care access this time… certainly surprised us, but when you start thinking about the context of the past decade and the context of the pandemic in which you launched the survey, the findings are a bit less surprising.”
Callaghan said the rise of the opioid epidemic prior to the Covid-19 pandemic, and the growing recognition of the lack of mental health resources in rural America since the pandemic may be part of the reason. But changes in health care through the Affordable Care Act may have improved health-care access, bringing other issues to the top of the list, Callaghan said.
According to the U.S. Department of Health and Human Services, nearly 20 million people signed up for insurance as part of the Affordable Care Act during open enrollment this past year. During 2022, 35 million people signed up for insurance during the open enrollment period, 21 million of whom were part of Medicaid expansions.
Still the fact that mental health and addiction rose to the top across all categories was striking, he said.
“You’re going to see small changes in characteristics over the course of decades,” he said. “But the extent to which mental health and addiction have risen and were so consistently selected by stakeholders, demonstrates how big those issues really are.”
Stakeholders may have been focusing on what were the most pressing needs given the moment, Callaghan said. The survey was presented to stakeholders 2021. Partnering with rural health organizations like the National Rural Health Association, the Centers for Disease Control and Prevention, the American Hospital Association, and the National Association of Rural Health Clinics, the research center sent out links to the survey and asked stakeholders to comment. In addition, the center sent the survey to people who had filled out the survey in previous decades and asked stakeholders to identify others they felt may be able to provide insight.
According to the Pew Research Center, an estimated 40% of American adults suffered from increased mental health issues during the pandemic. A survey done by the Kaiser Family Foundation and CNN found that 90% of the American public felt the country was facing a mental health crisis. Adults across the country during the pandemic reported increased symptoms of anxiety, depression, hopelessness and sadness and suicidal ideation, as well as increased drug and alcohol use.
In all, 1,291 respondents answered at least one of the questions between July 2021 and February 14, 2022.
“I think part of (the rankings) could be that a lot of the rural stakeholders participating understood that we’re looking at 10 year trends,” he said. “Our data didn’t allow us to identify specifically why, for example, vaccination isn’t in the top 20 even though we might have expected it to be, due to the pandemic.”
Major concerns besides health-care access in previous surveys included heart disease and stroke, diabetes, and nutrition.
“We’ve seen some pretty considerable gains in heart disease deaths,” Callaghan said. “We still do have a gap between urban and rural America, but there have been some pretty considerable gains.”
Callaghan said it’s not clear if that is because rural health-care providers are better at managing the disease, or educating patients about the diseases, or if other topics have just become more important.
For now, Callaghan said, the study reveals where the focus of rural health systems should be, according to rural health stakeholders.
“We now have a better sense of the areas that are particularly in need of rural health investment,” he said. “We now know that addressing addiction and addressing mental health issues have become increasingly important to rural experts over the past decade and while health-care access remains important… we nonetheless have to start prioritizing the issues that are most important which are addiction and mental health.”
The Covid-19 pandemic has brought lasting changes to Vermont’s theater companies
A view of the outdoor Courtyard Theater at Northern Stage in White River Junction on Monday, June 5, 2023. Photo by Glenn Russell/VTDigger
At Northern Stage in White River Junction, crew members look at the weather forecast every morning to figure out if, between heat and rain, they will be able to work outside. The outdoor stage first built to adapt to the Covid-19 pandemic has become a permanent part of the setup.
When a reporter visited, the crew was busy setting it all up for the opening of “Sense and Sensibility,” the play the company is performing until July 9. All the sets were built in house, but that may not happen again. For the next play, “Twelfth Night,” which opens Aug. 1, half the sets are being built on site and half are being built a three-hour drive away by Upstate Scenic, a company in Chatham, New York, that constructs sets for theater and film.
Next season, the theater company will work with the contractor to figure out what makes sense to build on site and what makes sense to contract out.
The company experimented with this approach in March, with its production of “Sweat,” and “it went extraordinarily well,” said Jason Smoller, Northern Stage’s managing director.
Director of Production Brian Sekinger at Northern Stage. Photo by Glenn Russell/VTDigger
Northern Stage decided to outsource its set construction because space is tight and staff is hard to find, said Brian Sekinger, director of production. Upstate Scenic also works with Weston Theater Company and other local companies, he said
A lot of people, particularly in set construction, “pivoted to other careers” during the pandemic, Sekinger said. “They either went into more industrial construction or building houses or just sort of left and did something totally different.”
Set construction is just one of the ways that theater companies across Vermont have adapted in permanent ways to changes imposed by the pandemic. They have outsourced the work on sets, let theatergoers pick their ticket prices, and performed more outdoors in summer as they try to regain audiences that have yet to return to pre-pandemic numbers.
“The pandemic isn’t over,” said Cristina Alicea, managing creative director of Vermont Stage, which is based in Burlington but also produces a summer outdoor play at Isham Farm in Williston. “We’re still dealing with audiences not fully back yet.”
Assistant Lead Electrician Austin Bowles works backstage for the outdoor Courtyard Theater at Northern Stage in White River Junction on Monday, June 5, 2023. Photo by Glenn Russell/VTDigger
Reconstructing career pathways
Like Northern Stage, other companies have moved outdoors in summer.
Lyric Theatre Company in South Burlington adapted to outdoor plays for young audiences during the pandemic, and those have become part of the company’s regular programming, said Erin Evarts, the company’s executive director. In June, the company performed outside at three public libraries and at the Shelburne Museum.
Weston Theater Company also took its programming for children outside in 2021, and never went back. And, the company is also performing those plays in towns beyond its home.
“It’s now a free tour for audiences all over southern Vermont,” said Susanna Gellert, the company’s executive artistic director. The troupe perform for free outdoors in Grafton, Brownsville, Springfield and Rutland, transforming a show that used to reach about 800 people to one that reaches more than 4,000.
But the workers employed in the field of building those sets are fewer and farther between.
Sekinger said that, nationwide, about 30% of theater technicians went into other careers during the pandemic.
“So we’ve been starting to rebuild,” he said. “There just aren’t the same number of people that there were before.”
Early-career professionals, Sekinger said, did not get the same hands-on experience in college during the pandemic they would have before. For instance, they were not able to produce in person, on stage, because so much theater was on Zoom.
Between the shortage of experienced people and the lack of experience of new people, he said, the alternative to contracting work out would be to have staff members work 60 to 80 hours a week.
Full houses
The housing shortage is another factor leading to a dearth of technical professionals, Sekinger said. To alleviate housing costs for its employees, Northern Stage has bought some properties in the area and leased others, he said.
“During the pandemic, everybody moved up from New York, bought up all the housing and sort of stayed, which means there isn’t as much housing in the area for new people coming into the organization,” he said.
Smoller concurs: “It is becoming increasingly difficult to hire. It all comes down to housing.”
Weston Theater has taken another direction toward lowering housing costs for members of the company, at least in summer. It has formed a partnership with a company that in winter houses staff at Okemo Mountain Resort in Ludlow. That housing was not being used in summer, so Weston Theater is renting it.
A sign leans against a wall at Northern Stage in White River Junction on Monday, June 5, 2023. Photo by Glenn Russell/VTDigger
While outsourcing set construction, Sekinger said Northern Stage retains creative control over those sets.
“We just send them drawings and paint renderings and research images and say: ‘This is how we want it to look,’” he said. “And then it just shows up here.”
Josh Davis, Northern Stage’s technical director, goes to the shop in New York to make sure that it is building what was drawn, and to answer questions.
“And making sure that if they’re supposed to be painting something blue and we’re building something blue and those blue things touch each other, then it’s the same color blue,” Sekinger said.
Material differences
It’s a pretty significant shift in the industry right now, Sekinger said, for small regional theaters to acknowledge they cannot staff up the way they would pre-pandemic.
Sekinger said Northern Stage is adapting in other ways because materials are hard to get or cost more than they used to. He points to the painted plywood made to look like tiles on the floor of the outdoor stage set.
“We do a lot of painting wood to look like other other materials because it’s cheaper or easier to get wood than it is to get some of those other materials,” he said.
Another adaptation, Smoller said, is that Northern Stage is paying closer attention to what its audience wants. That change came about after the company staged “Spring Awakening” last year. The musical is about loss of innocence, abortion and teenage suicide.
“And the feedback we heard from people was it is just too difficult and too sad for this moment,” Smoller said. “So we thought oh, no, we can’t do sad plays anymore.”
Smoller said the company’s artistic director, Carol Dunne, considered pulling the next play, “Sweat,” but the company, proud to put the play on, decided to go ahead. The play deals with hard social issues, such as loss of jobs, poverty and addiction.
“This play deals with real issues, too,” said Smoller. “It is not about teen suicide, which is very difficult to grapple with.”
Smoller said it was universally well received.
“Our audiences loved it,” he said. “So many folks told us: ‘That is the best thing I have seen at Northern Stage.’”
The response reaffirmed that the company’s audiences still want challenging theater.
The Byrne Theater at Northern Stage in White River Junction on Monday, June 5, 2023. Photo by Glenn Russell/VTDigger
“They don’t want sad theater, necessarily, but it’s not that they just want to see ‘The Little Mermaid’ or ‘A Christmas Carol’ again,” Smoller said. “So what has changed for us permanently is we are really conscious of what people are looking for, and the season we are offering next season doesn’t have any ‘sad’ titles.”
That said, Smoller said, some people do want “A Christmas Carol,” and Northern Stage will offer a new adaptation of the play this year.
A push toward youth
If the pandemic led adults to avoid depressing plays, Smoller said young people are just looking for more in-person connection and belonging after years on Zoom, and so he is seeing increasing interest in the company’s intensive youth ensemble studios.
The studios offer students an opportunity to learn on the stage of a professional theater company, with professional actors, designers and directors.
In addition, he said, high school students are looking for inclusivity and belonging, and are drawn to theater by virtue of the fact that it is not closely associated with a particular gender.
“We don’t run a men’s lacrosse team,” he said. ”Even in high school, students who are grappling with their identity have to choose: ‘OK, if I’m going to be on the swim team, it’s the boys’ swim team or the girls’ swim team.’ And theater isn’t that. You never have to opt into one or the other.”
Teens tell him they find an inclusive place at Northern Stage, he said.
What does a ticket cost?
Another change brought about by the pandemic: Audiences are buying tickets at the last minute, said Evarts, at the Lyric Theater. She said the national trend is that tickets are being bought in the last week to 10 days before a show, and the Lyric is finding that, as well.
Alicea said Vermont Stage also contends with waiting for last-minute ticket purchases.
Last year, Weston Theater brought in another big change. Having trouble persuading people to buy subscriptions, it started letting patrons pick the price they want to pay for one. The company offered three prices for exactly the same seats. As a result, Gellert said, subscriptions doubled last year, and this year, the company had already sold more subscriptions before the season started than it did during the entire year last year.
This year, Weston Theater is also letting people pay what they will for previews — performances before a show is reviewed.
“You can choose to pay zero,” said Gellert.
Last year, Vermont Stage found that subscriptions dropped by half, and “I’m finding that a lot of people are still hesitant to sign up for a full year,” said Alicea. She believes the experience of the pandemic is leading people to wait and see before making long-term commitments.
“My hope is that people don’t wait and see too long, because it could spell trouble for our organization and others,” said Alicea.
This year, Vermont Stage, too, is letting people pay what they will for both subscriptions and individual performances. The company is letting patrons pay one of three prices — $24, $44 or $64 — for a general admission ticket. If people pay $64, they are helping to subsidize the people who pay $24, said Alicea.
Stage lights for the outdoor performance of “Sense and Sensibility” at Northern Stage in White River Junction on Monday, June 5, 2023. Photo by Glenn Russell/VTDigger
The company also offers three prices for subscriptions, with the same number of shows for each and also for general admission: $89, $149 and $209.
Based on early sales of subscriptions, most people are paying $149, Alicea said, which is what she assumed would happen. But the company thought the second-largest group would be people who paid $89, and that has not turned out to be the case. Instead, more people are buying at the $209 price, a sign that patrons want to support the organization, she said.
“They’re definitely showing up for us in that way,” Alicea said. “It’s deeply appreciated.”
Alicea said she was inspired to offer the pick-your-price model by Andy Butterfield, the marketing director at Weston Theater. Sharing information about what works is how theater companies hope to rebuild their field, she said.
Legislature shores up finances of emergency medical service providers around the state
As part of a larger budget deal, state legislators have approved $31 million in funding that will provide breathing room for the roughly 275 emergency medical services (EMS) statewide, some on the verge of collapse. The aid will be distributed in two batches, 40% possibly by October for emergency relief and 60% thereafterin the form of grants.
Renée Gray, the newly appointed Washington County manager and also the ambulance chief for Moosabec Ambulance Service in Jonesport-Beals, said the relief cannot come soon enough. One Washington County ambulance service closed earlier this year and others have merged due to low staffing and depleted revenues.
[irp posts=”25931″]
“The people that work in this field are problem solvers, and they’ll kill themselves trying to fix this problem. That’s basically what’s happened – EMS has finally revealed its holes,” Gray said.
The long-negotiated funding — EMS officials originally requested $70 million — got caught up in a legislative battle over a proposed budget addition to the governor’s $9.9 billion, two-year budget that was approved in March.
A blue-ribbon commission, formed last year to study the issue, made recommendations to the legislature. Rick Petrie, the interim executive director for Atlantic Partnership EMS, a statewide EMS collaborative, was a leading advocate in the effort to secure state funding.
“It’s not what we would have hoped because the blue-ribbon commission was pretty clear that EMS providers needed $70 million,’’ Petrie said. “OK, so we compromised, but now let’s turn this (money) out really quickly with very little red tape.”
How much red tape there might be is unknown because no further details about the allocations were announced. Also, the budget measure did not pass by a two-thirds majority that would have allowed it to go into effect immediately. The budget addition, which still needs the governor’s signature, passed 80-58 on Thursday in the House and by a 22-9 vote in the Senate.
Still, Petrie said approval of the funding indicates that lawmakers recognize providers are struggling and seem to understand that $31 million is merely a down payment toward building a better system.
Another promising sign, he said, is that the commission will reconvene, possibly this summer, to further assess EMS needs statewide.
House Speaker Rachel Talbot Ross in a statement agreed that access to emergency medical response services across Maine is an essential part of the state’s healthcare system that must be funded, although she did not say if that will be with continued state support.
“In some cases, it’s quite literally a life-or-death situation,” said Talbot Ross. “The funding in this budget will be a major step forward to help services stay open, attract new providers to the field and start the process of redefining what emergency medical services look like in Maine.”
The Maine Bureau of EMS, which operates within the Department of Public Safety, will be key in determining how the money is divided, according to Petrie. Maine EMS had urged lawmakers to support not only the emergency funding, but additional funds to assist EMS and ambulance services as they shift into new funding and operational models.
With few exceptions, EMS providers across all 16 counties have been largely, but inadequately, self-funded by low insurance reimbursements and small taxpayer contributions from individual cities and towns.
They are often staffed with underpaid EMTs, paramedics or volunteers.
[irp posts=”25984″]
Sam Hurley, the Maine EMS director, said that model is no longer sustainable. Although optimistic, Hurley agrees the devil is in the details.
“Maine EMS is excited that the governor’s office and Maine Legislature have identified the needs of the EMS system in Maine as a funding priority. That said, we too are anxiously awaiting the final action of the Legislature as to the specific language surrounding any funding introduced to the system,” Hurley said.
In May, Maine EMS released its 2035 EMS Vision & Plan, outlining what it sees as the steps needed to achieve true sustainability over the next 12 years for the state’s roughly 275 EMS providers that are operating at a loss or barely breaking even.
Many EMS providers are struggling due to a host of factors, including lagging reimbursement rates, recruitment and retention challenges, training, and an aging and rural population.
As a result, some services are routinely “out of service” when an ambulance can’t be fully staffed. Some other providers, such as Petit Manan in Washington County, which served Milbridge and Steuben, have ceased operations.
But it’s not only rural EMS providers that are suffering.
A University of Southern Maine national study released in May by the Maine Rural Health Research Center revealed that 15 of the 16 Maine counties have so-called ambulance deserts, where people are located more than 25 minutes from an ambulance station. In the Northeast, Maine was ranked as the second-worst ambulance desert state, behind only Vermont, where every county contains at least one.
Only Androscoggin County has an adequate number of ambulance stations to provide reliable, fast responses. Even higher-density counties such as Cumberland, encompassing Portland and its environs, and Penobscot, which includes Bangor, have pockets that lack adequate ambulance response times, according to the MRHRC geographic disparities study.
Petrie said he got a call this past week from the service chief for “a fairly large metropolitan department in the state,” saying they were drowning in overtime expenses trying to cover the increasing number of calls and mutual aid requests. Petrie said the money would be allocated to any EMS department providing 911 response that shows it needs help — even metropolitan departments.
He said that the situation in rural communities is even more dire. Petrie said he knows that in places like Washington County and Aroostook County — virtually anywhere north of Augusta — EMS departments are “barely there” and doing everything they can to hold on.
“This money will be a lifeline to them while we work out the longer term,” Petrie said.
He and other EMS officials said the solution is multi-pronged, requiring state assistance, better insurance reimbursements, realistic financial contributions from municipalities being served and a more regional approach, with fewer, more robust, strategically located providers.
That assessment was echoed by Yvonne Jonk, associate research professor at the University of Southern Maine and deputy director of the Maine Rural Health Research Center. Jonk, the lead researcher for the ambulance deserts study, said the data proves that regionalized services are needed, particularly in rural areas with large geographic footprints and low populations.
“With regionalization you’re able to triage and determine the optimal location of an ambulance service, and to have each other’s backs instead of all this ad hoc community goodwill,” Jonk said.
Slowly, EMS providers and municipalities are heeding that warning, organizing and financially supporting regional services such as the new Bold Coast EMS department in Washington County, pressed into a regional model out of necessity after the closure of Petit Manan and regular staffing shortages in the Cherryfield ambulance department.
Bold Coast EMS opened June 12 with an inter-local agreement between the towns of Cherryfield, Milbridge and Steuben, each paying an equal share of the roughly half million-dollar annual operating budget. The smaller outlying towns of Beddington and Dubois kick in a donation for their coverage.
Mariah Curtis, the former Cherryfield service chief who is also a full-time nurse, is service chief for the new consolidated ambulance department. She said they are entirely taxpayer funded and didn’t bank on getting any state support.
“We built it to be self-sufficient, just with our community supporting us, and they’re very receptive to that,” Curtis said. “We will be open and appreciate anything we can get that makes the burden less on our taxpayers, but we don’t need it to bail us out.”
Bold Coast employs four full-time people during the day and uses part-time, on-call EMTs at night. The pay is $20 an hour for an EMT with 100% employer-paid health insurance and a zero deductible policy, all of which Curtis said keeps morale high.
The regional service is the second of its kind in Washington County; the first was Downeast EMS, which serviced the far eastern half of the county, with nine ambulances out of bases in Baileyville, Lubec and Eastport. Answering about 1,900 calls last year, Downeast EMS has operated in the black for the past decade.
Regionalism advocates say the local examples show there is strength in numbers. Data presented to the blue ribbon commission showed that of ambulance services performing less than 1,800 calls per year, most run less than 500, losing roughly $2,000 per call, largely due to poor insurance reimbursements.
Seventy percent of all ambulance runs in Maine are paid for by Medicare or Mainecare. Those services only reimburse 85 percent of the cost.
But there also is a glimmer of hope on that front coming out of the Legislature. Private insurers will begin paying higher reimbursements, according to Petrie. He’s hopeful that the next session and the blue-ribbon commission will make changes to the government reimbursement rates as well. He said that is critical, especially in places like Washington County.
“I believe that the blue-ribbon commission coming together again will start to attack those issues, or start down that pathway,” Petrie said. “They are going to have to come up with a fairly significant, radical way to deliver EMS up there — and the hospitals need to be involved as well.”
Sign up for the Downeast Monitor, a free newsletter produced by The Maine Monitor, to stay informed of what’s happening in Washington County.
In the year after Roe fell, out-of-state abortion patients did not flock to Vermont
Maddie Corkum listens as speakers address several hundred people gathered at the Unitarian Universalist Church in Burlington after the U.S. Supreme Court overturned the Roe v. Wade abortion decision on Friday, June 24, 2022. Photo by Glenn Russell/VTDigger
Defying the predictions of abortion advocates, providers and state lawmakers, the number of out-of-state patients who traveled to Vermont to obtain abortions did not increase, but in fact dropped, in the year after the U.S. Supreme Court overturned Roe v. Wade case precedent, according to preliminary data from the state Department of Health.
When the court’s conservative majority issued its Dobbs v. Jackson Women’s Health Organization decision last June, the country became a patchwork of disparate reproductive health laws. In states with so-called trigger laws, abortion was severely restricted or outright banned once the decision was issued. Other state legislatures, emboldened by the court ruling, worked quickly to impose new restrictions on the procedure in their respective states.
Vermont lawmakers had seen a post-Roe future coming, and proactively worked to expand access to abortion within Vermont’s boundaries — not only with Vermonters in mind, but also for out-of-state patients who they foresaw traveling from their respective states to obtain the procedure.
Experts never expected a tsunami of out-of-state patients, largely because Vermont is a remote, rural state that can be difficult or cost-prohibitive to travel to from far distances. When the high court issued its Dobbs decision, Planned Parenthood of Northern New England predicted a modest 10% increase in out-of-state patients.
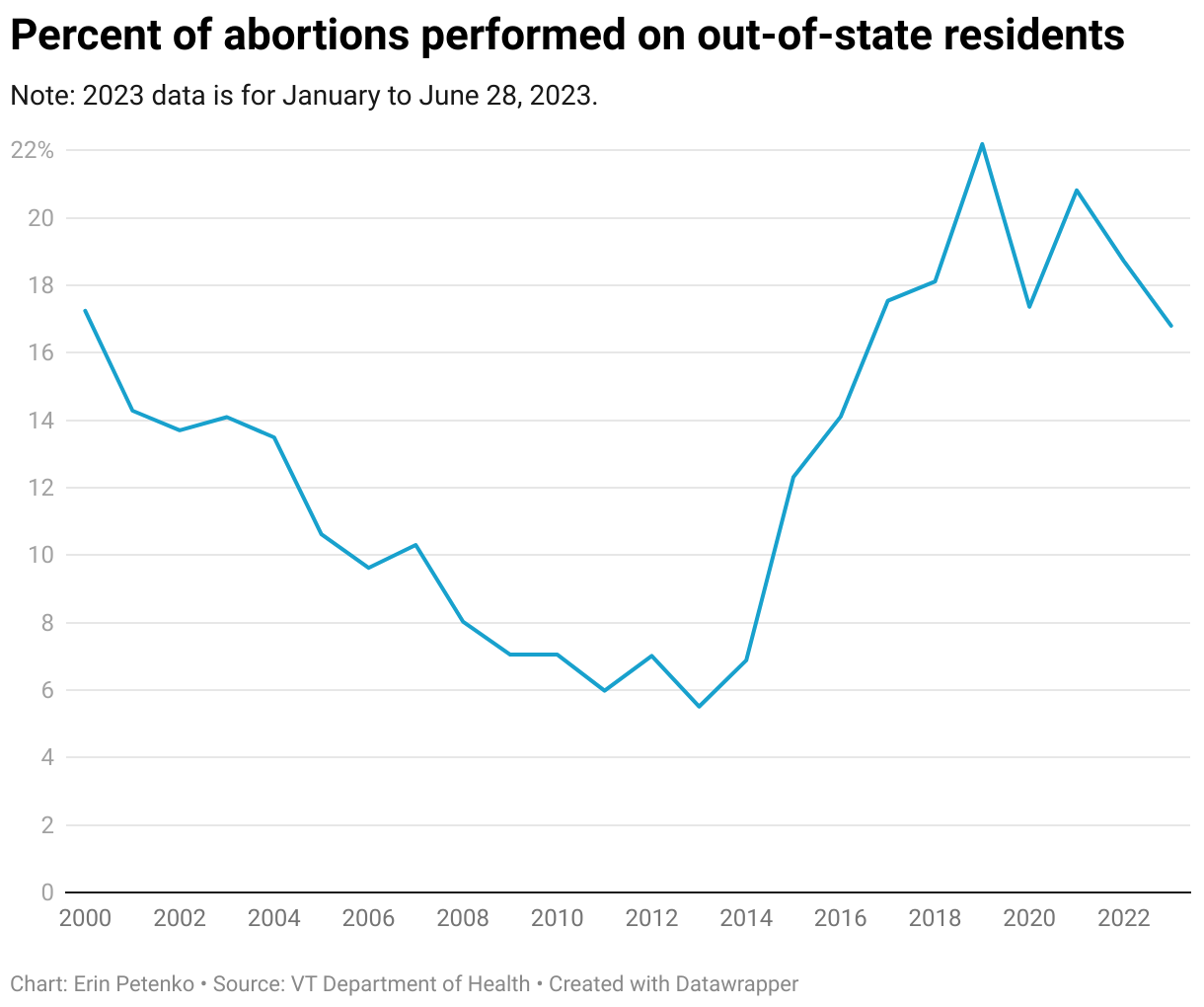
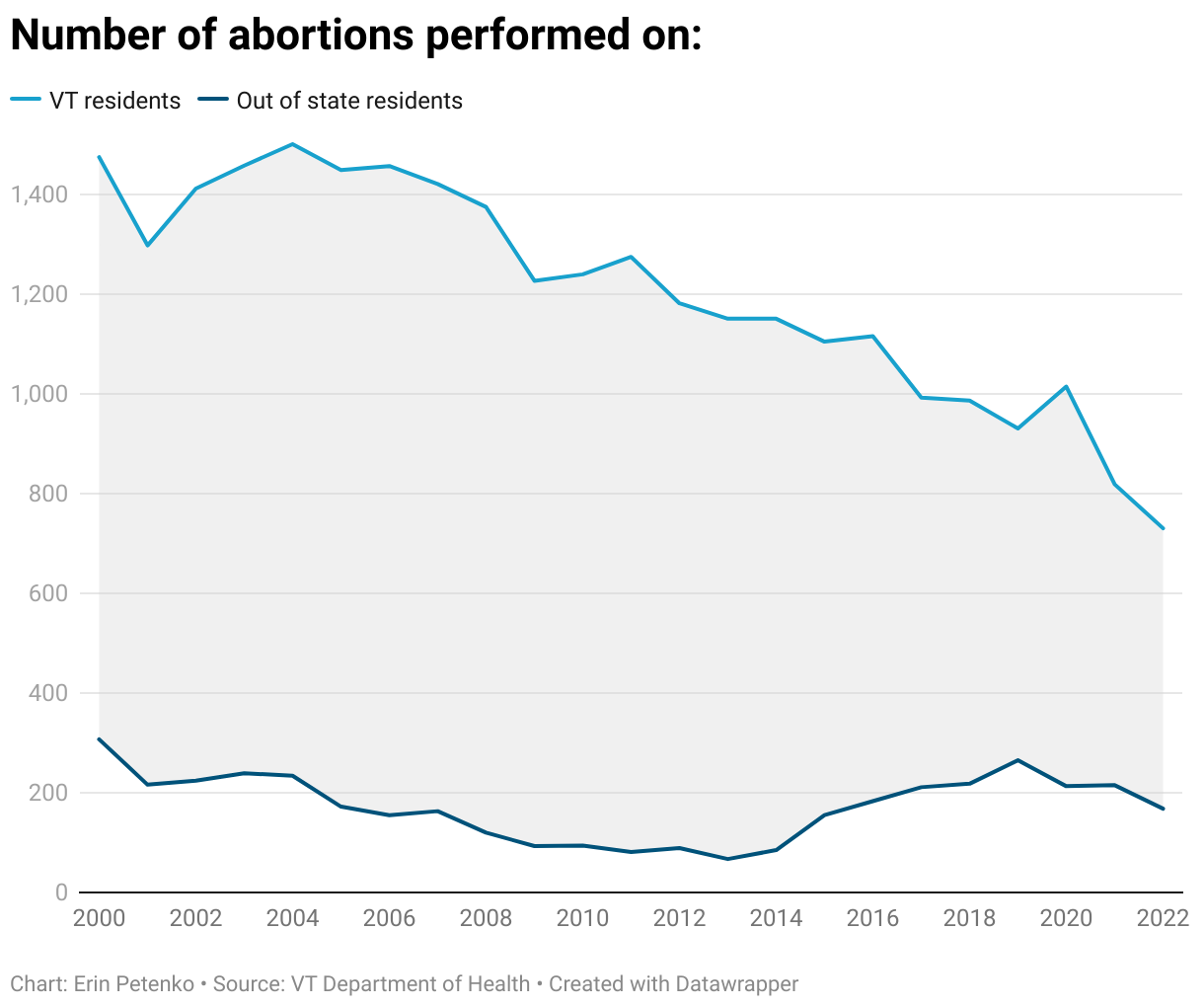
But according to preliminary data that VTDigger requested from the Vermont Department of Health, even that didn’t come to pass. As of this week, the department reports that from June 24, 2022 — the day of the Dobbs decision — through early June 2023, a total of 925 abortions were completed in Vermont. Of those, 154 were performed on non-Vermont residents — roughly 17%. (Due to reporting lag time, the department was unable to provide data from the latter portion of June 2023.)
By comparison, in all of 2021, 215 out-of-state patients obtained abortions in Vermont, representing nearly 21% of the 1,033 abortions completed in the state that year.
Since 2018, the proportion of out-of-state patients who obtain abortions in Vermont has remained relatively stable, hovering between 17 and 22% every year. But mirroring national trends, the total number of abortion patients in the state — both those who hail from Vermont and those who don’t — has trended downward.
In the year since Roe fell, a handful of patients traveled to Vermont from far-flung states where an abortion is difficult to obtain: Alabama, Louisiana, Tennessee and Texas, to name a few. But most out-of-state patients traveled from nearby states, where access to abortion is, in theory, about on par with Vermont: Connecticut, Maine, Massachusetts, New Hampshire, New York and Rhode Island. More than half of all out-of-state patients came from New Hampshire, mirroring past years’ trends.
Vermont’s clinics had anticipated such a trend, according to Lucy Leriche, vice president of Vermont public affairs for Planned Parenthood of Northern New England. “There are a lot of reasons why people from out-of-state are getting an abortion in our region,” she said, speaking of Vermont as well as New Hampshire and Maine.
Sometimes northern New England is where the patient has a family member or support system to assist in the process, Leriche said. Perhaps they are fleeing a domestic violence situation. They could be attending college here, but a legal resident elsewhere. Maybe they just want more privacy. Or perhaps, if they hail from a nearby state that has more patients, such as New York or Massachusetts, they couldn’t get an appointment at home. A domino effect in appointment availability can ensue, Leriche said.
Planned Parenthood — the largest provider of abortions in Vermont, and nationwide — declined to provide state-specific data on its own out-of-state patients, citing concerns over patient privacy and safety. But in Maine, New Hampshire and Vermont combined, the organization earlier this month reported a 12.5% increase in out-of-state patients “seeking abortion at our health centers,” according to a June press release.
Beyond patient data, Leriche said the impact of the Dobbs decision was palpable in other ways. Planned Parenthood of Northern New England’s call center was “inundated” immediately after the ruling was made, she said. Online, the organization’s website had its largest one-day spike in web traffic on June 24, 2022, the day of the court’s ruling. “That is, I think, a really strong indicator of the response,” Leriche said.
The Dobbs decision “is very destabilizing and very anxiety-producing, and causes a lot of confusion and anxiety and fear and panic,” Leriche said.
Leriche said the organization is trying to keep its messaging on target, emphasizing that abortion remains legal in Vermont. This legislative session, state lawmakers passed landmark shield laws protecting Vermont-based abortion providers — and to some extent, patients who travel to the state — from out-of-state abortion prosecutions or investigations.
Lack of mobile clean needle exchange hampers HIV mitigation in eastern Kanawha County
On a hazy summer afternoon, a silver pickup truck rolled into a parking lot filled with pop-up tents in Charleston’s Kanawha City. As it came to a stop, four people from Marmet experiencing homelessness hopped out and began walking around a free wellness event.
Social service providers from around the county had gathered to help people like Pamela Hale, one of the Marmet residents. She was grateful for the resources available, ranging from hot lunches to basic first-aid care to HIV testing.
Hale, who referred to herself as the encampment’s “mama,” wished more people had joined her. But she said they’re often skeptical of social service workers who come by, like the ones who gave Hale a ride to the event.
“They think automatically, ‘cops,’” she said.
This community wellness event is one way health providers are trying to build bridges to eastern Kanawha County communities like Marmet, areas they’ve struggled to reach in the past. State and local infectious disease experts say this region has been among the most impacted by the effects of the county’s injection drug use crisis, including HIV, hepatitis C and endocarditis.
Health workers know an effective strategy for building relationships here, one that’s worked well in neighboring Fayette County: mobile syringe service units. These operations could be regularly set up near encampments, providing disease testing and also letting people exchange used needles for sterile ones.
“I think the high-risk group would come out for that,” said Christine Teague, the director of Charleston Area Medical Center’s HIV Care program.
But West Virginia lawmakers passed a law in 2021 granting local governments the power to approve and revoke the authorization of needle exchanges. And in Kanawha County, commissioners have only authorized one program — which operates in Charleston and is difficult for people in towns like Marmet, Rand, Belle and Montgomery to reach without reliable transportation. They’ve indicated they don’t see a need for more than one exchange in the county.
“I wish to God we could have a mobile syringe unit,” said Cassie Province, an outreach worker at the nonprofit Covenant House. “But they won’t let us do that.”
Charleston Area Medical Center and Manna Meal Soup Kitchen set up their mobile trucks at a Kanawha City free wellness event. Photo by Allen Siegler
How we got here
The U.S. Centers for Disease Control and Prevention has repeatedly found that syringe service programs decrease infectious disease transmission and reduce needle litter. But the vital tool has faced pushback operating in Kanawha County for years. Since 2018, two programs have closed after both Charleston and West Virginia passed policies restricting syringe exchanges.
The 2021 state law stipulated how the programs could operate and gave county commissions and city councils the power to approve and close them. Health professionals at both the national and state levels worried about how these closures and others across the state would impact people who inject drugs. Charleston and Huntington were already in the midst of large injection drug-use HIV outbreaks, with a top CDC official calling Charleston’s the country’s “most concerning” outbreak of the year.
Outside of West Virginia’s two largest cities, rural spread was also expected. And data from Charleston Area Medical Center supports that, at least in Kanawha County, it’s been happening. Maps from the hospital system indicate that from 2017 to 2021, people in the county’s more rural, eastern parts have been at high risk of hepatitis C and HIV.
Teague said that region and Charleston’s West Side are the areas in Kanawha County most affected by diseases transmitted via used syringes. Unlike their efforts in the West Side of Charleston, her program and other health services have struggled to test and treat eastern Kanawha County residents — leading Teague to believe the HIV and hepatitis C case numbers in the area are significantly higher than official numbers indicate.
“This high-risk group may not be interested in coming out unless you have something useful for them,” Teague said. “Whether that’s syringe service programs or food or what have you.”
While the 2021 state law limits when and where mobile needle exchanges can operate, it does allow for them to exist. Robin Pollini, an infectious disease epidemiology professor at West Virginia University, said syringe service programs that are able to travel to small, rural eastern Kanawha communities would help mitigate HIV and hepatitis C spread.
“People who use drugs have traditionally not had good experiences with the health care system,” she said. “That’s why having a mobile unit, which is very different from having them come into a medical setting, is so important.”
But the law also requires approval from the county commission for any needle exchange program to operate. Kanawha’s commissioners have only authorized one program: West Virginia Health Right.
The free clinic runs its needle exchange program solely from Charleston and does not offer mobile services in the county. 2022 data from the state health department indicates Health Right distributed far fewer sterile needles than programs in Huntington and Morgantown.
In 2021, Angie Settle, the clinic’s executive director, told the Kanawha County Commission her organization’s needle exchange policies create “a multitude of safeguards” to make sure every syringe is returned. In that same meeting, she said Health Right does not plan on expanding its program. Settle did not respond to a phone call or an email asking whether those plans have changed.
From left, Kanawha County Commissioners Ben Salango, Kent Carper and Lance Wheeler at a press event earlier this year. Photo courtesy the Governor’s Office.
In previous interviews, Kent Carper, president of the Kanawha County Commission, has said Health Right offers enough syringe exchange services for the county. When presented with multiplestudies indicating that Kanawha would benefit from easier access to needle exchanges, he has questioned the researchers’ intentions and credibility. A spokesperson for the county said Carper and Ben Salango, a fellow commissioner, were both unavailable to comment for this story.
In a phone call, Lance Wheeler, the third commissioner, did not indicate whether he would support mobile syringe service programs in the county. He said he relies on administrators at Health Right and the Kanawha-Charleston Health Department to tell him and other local elected officials what the needs are to address the opioid epidemic.
Without any other authorized programs, no one else can legally offer that service. As a consequence, government decisions that helped diseases spread in eastern Kanawha County also hinder health professionals from using one of the most effective tools to mitigate it.
“Right now there is not sufficient capacity for the need in Kanawha,” Pollini said. “Or almost anywhere, really. But particularly in Kanawha.”
What a syringe exchange could do for Kanawha County
In Smithers, a town of just over 700 people on the border between Kanawha and Fayette counties, a mobile syringe service program shows the impact that one could have in eastern Kanawha County.
The county border runs through the town, and there’s little visible difference between the two sides. But, unlike Kanawha County, Fayette County Commissioners have authorized its health department to run a mobile needle exchange unit in the area. So, twice a month, Fayette County Health Department peer recovery specialist Paula McCutcheon travels to the Fayette side of Smithers and sets up a needle exchange for a few hours.
Her primary goal with the unit is to make testing and comprehensive harm reduction services as accessible as possible to any West Virginian who needs it.
“They can’t come to us, so we’re going to come to them,” McCutcheon said. “Our goal is to keep them alive and safe and meet them where they’re at.”
The Fayette Health Department program can only show up at specific times and places approved by the state. But to Brooke Parker, a clinical social worker with CAMC, McCutcheon is using the mobile exchange to create the type of trust the hospital’s HIV care program yearns to build with residents in eastern Kanawha County.
“She’s really out there in the community, and she knows exactly what needs to be done,” Parker said.
It’s the type of effort Pollini believes is crucial for the Upper Kanawha Valley, regardless of which side of the Fayette-Kanawha border someone happens to live in.
“That kind of service can be much more effective than just going in and doing testing,” she said. “Because you’re building those relationships.”
Bennington ambulance service and recovery center team up to reach drug users
Bill Camarda, executive director of the Bennington Rescue Squad, staffs a booth at the annual MayFest event, providing harm reduction materials and education to members of the community. Photo courtesy of Bennington Rescue Squad.
The Bennington Rescue Squad and the Turning Point Center of Bennington have launched a new kind of partnership to reach people with substance use disorders who have so far been falling through the cracks. The Vermont Office of Emergency Medical Services calls it the first collaboration of its kind in the state.
Whenever the rescue squad responds to a substance-related call – many of them nonfatal opioid overdoses – emergency responders offer to take patients to the local emergency room, where volunteer peer coaches with the Turning Point Center are on standby to talk about paths to recovering from substance abuse.
But of the 20 to 30 emergency calls the squad receives every month, at least 25% of the patients refuse to be taken to the hospital, said squad director Bill Camarda. For those five to 10 people, emergency responders can only leave them with opioid antidote kits and printed information about where to seek help.
“They really don’t want to have anything to do with the health care system,” Camarda said. “But at the same time, they’re not in the right mindset to be like, ‘I really need some help right now.’”
He said those patients are deterred by several factors: the stigma attached to drug use, a belief that nothing can help them, or preoccupation with getting their next dose, which will get rid of withdrawal symptoms.
After seeing dozens of local residents with substance use disorder fall through cracks in the system each year, the two Bennington nonprofit organizations decided to partner on another way to reach them.
Starting June 9, when someone who shows signs or a history of substance use disorder refuses to be taken to the emergency department by the Bennington Rescue Squad, Camarda said paramedics on scene ask for written consent to share the patient’s name, contact information and case summary with the Turning Point Center.
If patients agree, peer coaches will visit them within 24 to 48 hours and discuss the resources available in combating substance use disorder.
Bennington EMT Rick Noel preparing harm reduction kits to hand out for at-risk individuals and at public events. Photo courtesy of Bennington Rescue Squad
“We have the opportunity to potentially get ahead of some of these crises,” said Margae Diamond, executive director of the Bennington Turning Point Center.
Like they do at the hospital emergency room, the coaches may discuss medication-assisted treatment, psychotherapy, recovery coaching, support group meetings and organizations that can help with finding work or a new home.
During these home visits, Diamond said, recovery coaches will pair up with a local mental health professional from United Counseling Service, in recognition that substance use and mental health are often closely linked.
On top of the growing number of opioid overdose deaths, the Bennington recovery center is also concerned about the pervasive use of alcohol. The state Department of Health has reported that last year in Vermont, excessive alcohol use was associated with nearly one in four deaths among people ages 20-34 and nearly one in five deaths of those ages 35-49.
ALCOHOL-RELATED DEATHS AMONG VERMONTERS
“The ricochet of problems that develop from long-term alcohol use is something that we’d like to be able to identify earlier and provide some connection to resources,” Diamond said.
Since the partnership’s launch in June, however, only three patients have allowed the rescue squad to share their information with the recovery center. The leaders of both organizations say they’re working on strategies to increase participation, such as fine-tuning how their staffers communicate with patients.
Still, the state EMS Office lauds the initiative, saying it’s a model for other Vermont communities.
“The seriousness of the opioid crisis and increasing number of overdoses and deaths necessitates innovation and locally developed solutions,” said Bambi Dame, the state health department’s emergency medical services chief.
She said some groups in Chittenden County are already discussing setting up a similar partnership.