With no opposition in the room, a rural Texas county makes traveling for an abortion on its roads illegal
Cochran County, which borders New Mexico, joins a small group of other rural Texas counties that have passed these ordinances. Abortion-rights supporters say the new policies are not legal.
Post-Roe, North Dakota puts resources into alternatives to abortion
North Dakota this year adopted one of the strictest abortion bans in the country, with narrow exceptions for rape and incest victims in the first six weeks of pregnancy and to save the life of the mother.
Although abortions-rights advocates haven’t given up the fight, abortion opponents are moving ahead with the restrictions and placing a heavier emphasis on supporting new mothers through legislation and services, such as maternity homes for pregnant women and teens.
Molly Richards, 17, hugs her son, Bernard. Richards lives at the Saint Gianna & Pietro Molla Maternity Home, which provides services to pregnant people. (Photo courtesy of Molly Richards)
One of those teens is Molly Richards, who was just 13 years old when she learned she was pregnant.
She remembers feeling both “excited and oblivious” when she got the results at a clinic on the Pine Ridge Reservation in South Dakota, where she grew up. The community is home to the Oglala Sioux Tribe, of which Richards, now 17, is a citizen.
“It was a very happy time for me,” she recalled.
Then the reality of carrying and raising a child began to sink in. But Richards didn’t view abortion as an option.
“Abortion was not on my mind. That was a big no-no for me.”
Seeking resources, Richards and her family connected with Mary Pat Jahner, director of Saint Gianna & Pietro Molla Maternity Home in the small, unincorporated community of Warsaw.
The picturesque brick home – four stories tall and trimmed with ornate gold crosses – is an institution within the North Dakota anti-abortion movement.
Originally a convent for nuns and a boarding school, the home now serves young pregnant women – most from nearby Native American reservations. In addition to food and shelter, the facility provides counseling services, help completing high school, clothing, job training and parenting classes to mothers.
The facility houses two to four residents at a time. Richards was four months into her pregnancy when she arrived at the home.
“Our main purpose is just to provide a choice for moms who …might need a place to stay or might need a family,” Jahner said. “Most of the moms don’t have a safe place to be, they might be living couch to couch. They’re not living on the street per se, but they might not have their own place to call home.”
Saint Gianna & Pietro Molla Maternity Home, seen here on July 6, 2023, is an institution within the North Dakota anti-abortion movement. Located in Warsaw, the facility was originally a convent for nuns and a boarding school. It now serves young pregnant women. (Trilce Estrada Olvera, News21)
With abortions essentially unavailable in the state, where religion is deeply ingrained and diverse, efforts to support mothers and their children have taken on new prominence.
After the U.S. Supreme Court overturned Roe v. Wade in 2022 and returned abortion decisions to the states, researchers predicted the number of births would increase, as would the need to support pregnant people, young mothers and their children.
An analysis by the Johns Hopkins Bloomberg School of Public Health estimates that nearly 9,800 additional live births occurred in Texas from April 2022 through December 2022 after a six-week abortion ban took effect in that state in fall 2021.
The federal Congressional Budget Office has said it anticipates an increase in births because of the end of Roe but that contraceptive use and other abortion methods, such as medication abortion, will largely offset that increase.
Kathy Hirsh-Pasek, a psychology professor at Temple University and senior fellow at the Brookings Institution, doesn’t think the United States is prepared for an influx of births – and that policies nationwide aren’t doing enough.
“We are right now not a family friendly country. We may be pro-life, but we’re not pro-family. And if you’re going to make decisions that put more babies into the market, we need to support those babies,” she said. “I don’t care if you’re pro-Roe or anti-Roe, support children. They’re your future.”
Supporting pregnant people through legislation
State Sen. Sean Cleary, R-Bismarck, has been at the forefront of pushing for additional help for mothers and babies amid North Dakota’s abortion ban.
Sen. Sean Cleary, R-Bismarck, talks in the North Dakota Capitol in Bismarck on July 10, 2023. He pushed for legislation supporting mothers and children. “This topic was definitely top of mind for a lot of folks with the Dobbs decision.” But, he said, “These are all ideas that I would have supported either way.” (Morgan Fischer, News21)North Dakota this year adopted one of the strictest abortion bans in the country, with narrow exceptions for rape and incest victims in the first six weeks of pregnancy and to save the life of the mother. (Morgan Fischer, News21)
“There was an understanding that women are navigating a very difficult time in their lives, that the state could be doing more to support them and empower them,” Cleary said. “We wanted to be a state that was known for supporting families and supporting mothers.”
Cleary co-sponsored the diaper tax and Medicaid bills, as well as failed efforts to create a paid family leave program, a tax credit for child care expenses and a program to increase pay for child care workers.
The 31-year-old said being a father helped him see the need for this type of legislation. He has a toddler and another child on the way.
“Families can’t afford to send their kids to child care, and the workers can’t afford to work there,” he said.
Abortion-rights activists doubt the effectiveness of the few measures that made it through the Legislature.
“None of them are actually adequate to address fully supporting a pregnant person bringing a child into the world and raising a child to adulthood,” said Cody Schuler, advocacy manager for the American Civil Liberties Union of North Dakota.
“If you’re going to have a near-total ban on abortion and you’re going to force people to carry pregnancy to term, you have to do more than give a tax break for diapers.”
Katie Christensen, North Dakota state director for Planned Parenthood, emphasized the problematic funding of the alternatives-to-abortion program.
Katie Christensen is the North Dakota state director of external affairs for Planned Parenthood North Central States. Though Planned Parenthood does not provide abortions in North Dakota, it is part of an abortion-rights coalition in the state. (Trilce Estrada Olvera, News21)
Christensen has criticized the program for providing $1 million in state funds to mostly religious ministries with little to no government oversight. State funding for so-called “crisis pregnancy centers,” which aim to dissuade people from getting abortions, is especially concerning to abortion-rights advocates.
There are at least seven such centers in the state, according to the Crisis Pregnancy Center Map, which provides nationwide tracking of these facilities and is maintained by University of Georgia professors.
“We’re putting thousands of public dollars into programming that aims to seek out people who want abortions and try to persuade them away from that,” Christensen said. “They’re still allowed to promote their religion while using these dollars.”
Despite this criticism, Sen. Tim Mathern, D-Fargo, one of only four Democrats in the 47-member state Senate, co-sponsored the alternatives-to-abortion funding bill, claiming that it “sort of became a litmus test between pro-choice and pro-life people.”
Although he supports abortion access, Mathern backed the bill in an attempt to change the tide of Democrats in North Dakota being seen as “the anti-religion and anti-God people and the people who kill babies.”
However, if concerns over these “crisis pregnancy centers” are legitimate, Mathern said, their practices should be evaluated and “the state’s attorney should be investigating.”
‘Small government’ approach to helping mothers
North Dakota’s Legislature meets for 80 days during odd-numbered years only. Legislators, who don’t have staff, work at their desks on the floor of the Senate or House. This model can mean less government funding for programs, something Republican state Sen. Janne Myrdal supports.
Myrdal represents far northeastern North Dakota, where the Gianna & Pietro home is located. She sponsored the state’s strict new abortion ban and co-sponsored the bill that beefed up funding to the state’s alternatives-to-abortion program. She warns that such funding comes with some strings attached.
“If you ask for that much support, then the government’s going to come on top of it and go, ‘We’re going to regulate you,’” Myrdal said. “You can’t pray for people, you can’t hug people, you can’t share Jesus with people who come in, because the government can’t do that.”
Gianna & Pietro, which is a nonprofit organization, receives the majority of its funding – about $500,000 to $600,000 each year – from individual donors, but it also has received funds from the state’s alternatives-to-abortion program.
In this year’s bill, about $100,000 was earmarked for the home; Jahner said the money will go toward updating vehicles and other needs.
In the nearly two decades of the home’s operation, more than 300 people have lived there, and over 100 children have been born as part of the program.
During a recent visit, three women who were either pregnant or young mothers, including Richards, lived at the home. Staff members stay on site, too, to provide support and help.
Jahner, her daughter, whom she adopted from a former resident, and several other children of former residents live on the property, as well, in a two-story home behind Gianna & Pietro.
Molly Richards, 17, feeds Brooklyn, another resident’s baby, on July 5, 2023, at Saint Gianna & Pietro Molla Maternity Home in Warsaw, North Dakota. Richards and other mothers living at the home help care for the children. Richards is in the process of having her own son, Bernard, adopted by a family in southern Minnesota because, “I wanted something more and better for my son,” she said. (Morgan Fischer, News21)
Richards’ initial stay in 2019 only lasted a month. Feeling homesick, she returned to South Dakota to give birth. But after struggling to parent on her own and dropping out of school, Richards returned to Gianna & Pietro over a year and a half ago, with her son, Bernard, in tow.
Richards is now in the process of having her son adopted by a family in southern Minnesota, because, she said, “I wanted something more and better for my son.”
There is a clear religious aspect to Gianna & Pietro. Residents must attend Sunday Mass, take part in nightly prayer and participate in grace before meals. A stained glass chapel is located on the first floor of the home, and delicate religious paintings are scattered throughout. Across the street sits a steepled red brick church where residents may also attend Mass.
The Rev. Joseph Christensen holds Mass inside the Gianna & Pietro maternity home’s chapel on July 6, 2023, in Warsaw, North Dakota. Christensen holds Mass every day for the mothers and staff. (Trilce Estrada Olvera, News21)
Although residents are not required to be Catholic or religious to live at the home, a question about religious preference is included on the admission application form and participation in religious activities is required.
“I didn’t become religious until I actually came here, so my family isn’t religious,” Richards said. “I was baptized (Catholic) a year and a half ago.”
Schuler, of the ACLU, and other abortion-rights advocates worry such religious requirements could lead to “coercing individuals into religion” with the help of government funding.
“When it comes to a maternity home, it’s being operated as a religious ministry. I don’t think state dollars should be paying for that,” Schuler said. “But at the same time, I know that there are individuals who are religious who might be looking for what that center might provide.”
Expansion of reproductive care in Minnesota
With limited capacity in homes like Gianna & Pietro, abortion care across the Red River in neighboring Minnesota remains essential, abortion-rights advocates say.
“The amount of pregnant people who are having their abortions today across the river would fill up those homes fivefold today – unless they’re going to open up huge apartment complexes to house all of these pregnant people,” said Destini Spaeth, board chair of the North Dakota Women in Need Abortion Access Fund.
Abortion is legal in Minnesota up to fetal viability, which is 24 to 26 weeks, and exceptions are granted to save the life or protect the health of the mother. Surrounded by states that have completely banned abortion or are in court fighting to prevent access, Minnesota has become a key state for abortion access in the Upper Midwest.
For nearly 25 years, Red River Women’s Clinic operated in Fargo and was the only abortion clinic in the state for two decades. Every Wednesday, when the clinic was open, protesters gathered with graphic signs outside the front door.
Then last year, after word of the Supreme Court’s likely end to Roe was leaked, its operators began looking for a new location. Last August, they reopened less than 3 miles away – across the river in Moorhead, Minnesota.
Each Wednesday, the clinic provides 25 to 30 abortions up to the 16-week mark of pregnancy. After that time, patients are referred elsewhere for a multiday procedure that the independent clinic lacks capacity for.
Since the move, the clinic has seen its patient load increase 10% to 15%, said Tammi Kromenaker, the facility’s director. And with fewer overall restrictions on abortion care in Minnesota, Kromenaker said she believes access has actually increased for women in North Dakota.
But the fear her patients feel has also gone up, she said.
“Every week, mostly patients from North Dakota will say: ‘Is it even legal for me to come here? Will I get legally prosecuted for this health care?’
Kromenaker continues to fight for abortion rights back across the river in North Dakota. Her clinic is one of the plaintiffs in a lawsuit over the state’s near-total abortion ban.
“We didn’t want to give up on North Dakota. We didn’t want to leave,” she said. “But our hand was forced.”
News21 reporters Trilce Estrada Olvera and Cassidey Kavathas contributed to this story.
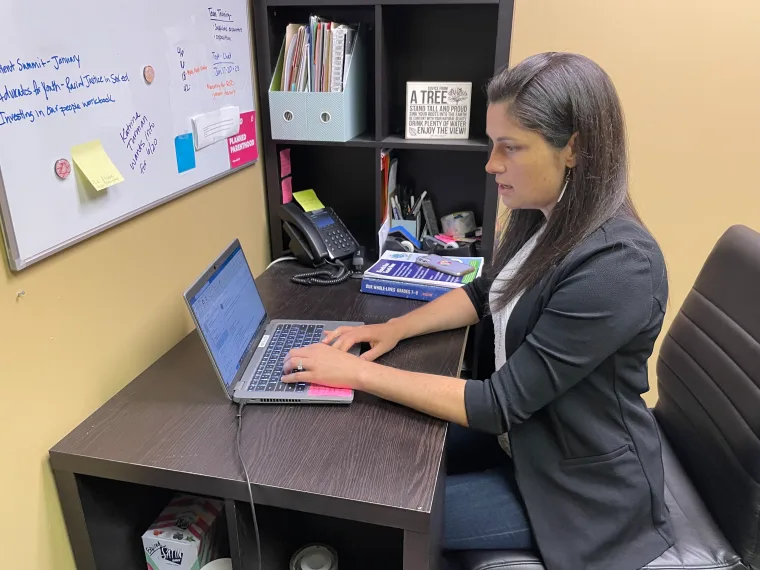
In the year after Roe fell, out-of-state abortion patients did not flock to Vermont
Maddie Corkum listens as speakers address several hundred people gathered at the Unitarian Universalist Church in Burlington after the U.S. Supreme Court overturned the Roe v. Wade abortion decision on Friday, June 24, 2022. Photo by Glenn Russell/VTDigger
Defying the predictions of abortion advocates, providers and state lawmakers, the number of out-of-state patients who traveled to Vermont to obtain abortions did not increase, but in fact dropped, in the year after the U.S. Supreme Court overturned Roe v. Wade case precedent, according to preliminary data from the state Department of Health.
When the court’s conservative majority issued its Dobbs v. Jackson Women’s Health Organization decision last June, the country became a patchwork of disparate reproductive health laws. In states with so-called trigger laws, abortion was severely restricted or outright banned once the decision was issued. Other state legislatures, emboldened by the court ruling, worked quickly to impose new restrictions on the procedure in their respective states.
Vermont lawmakers had seen a post-Roe future coming, and proactively worked to expand access to abortion within Vermont’s boundaries — not only with Vermonters in mind, but also for out-of-state patients who they foresaw traveling from their respective states to obtain the procedure.
Experts never expected a tsunami of out-of-state patients, largely because Vermont is a remote, rural state that can be difficult or cost-prohibitive to travel to from far distances. When the high court issued its Dobbs decision, Planned Parenthood of Northern New England predicted a modest 10% increase in out-of-state patients.
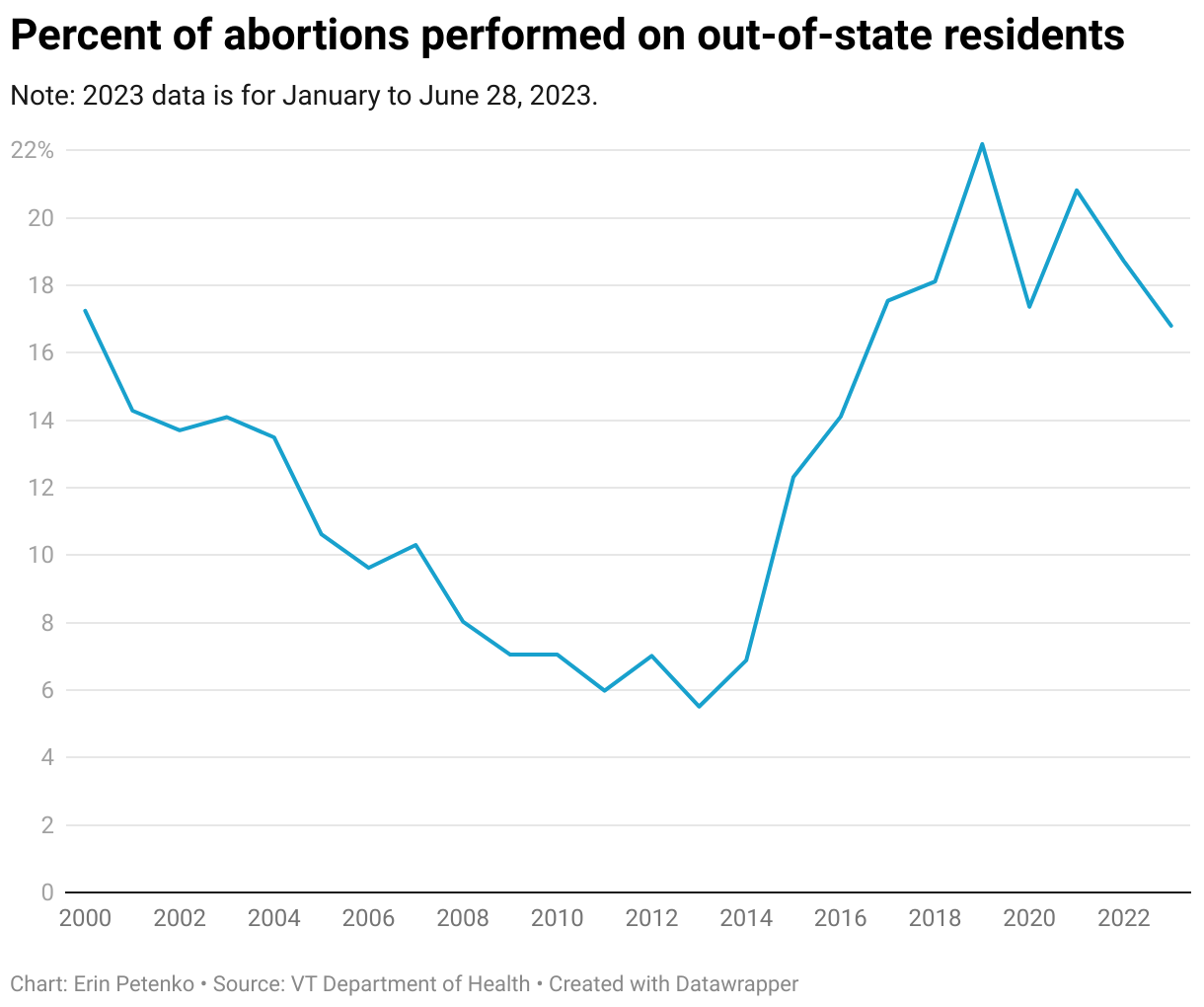
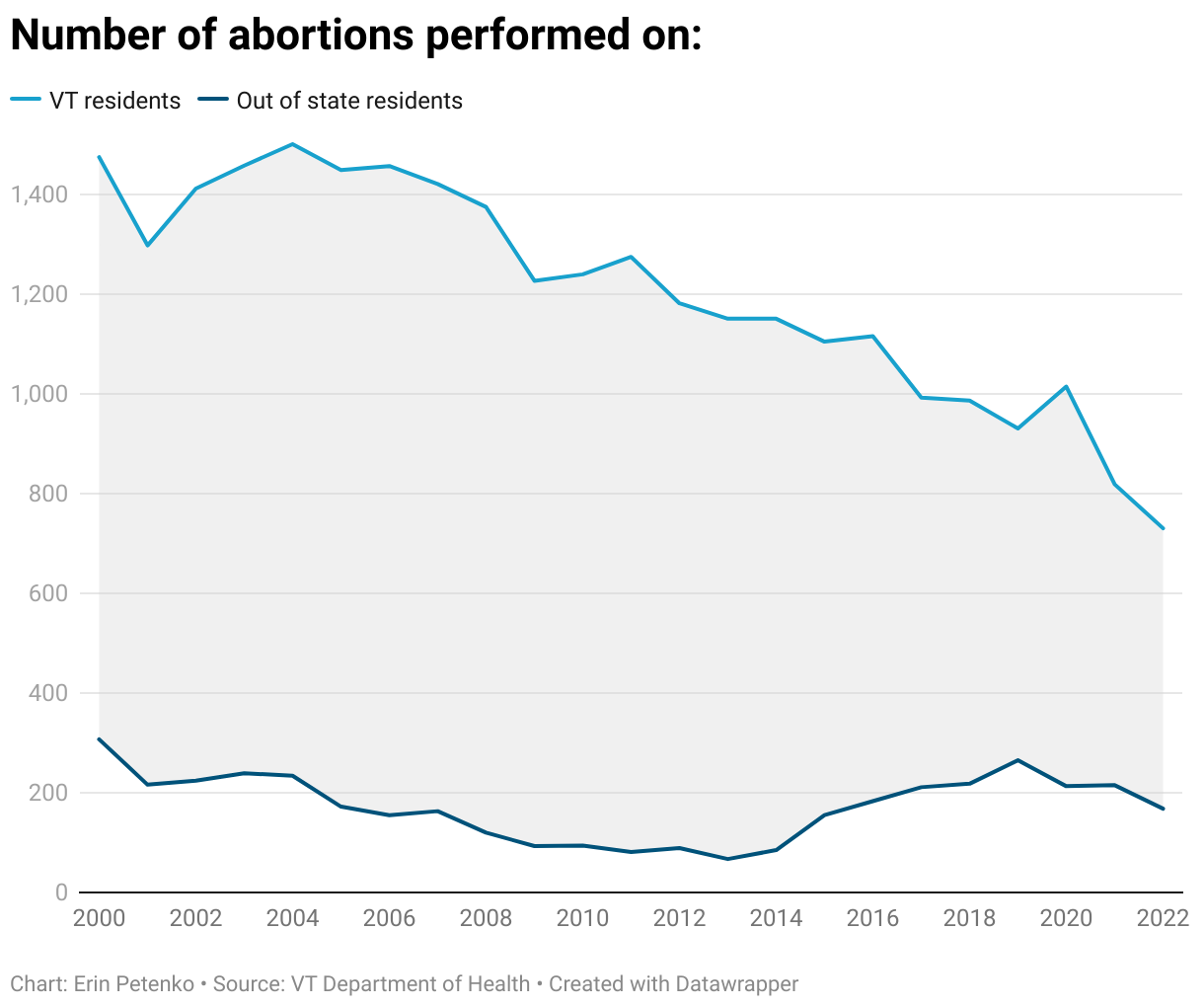
But according to preliminary data that VTDigger requested from the Vermont Department of Health, even that didn’t come to pass. As of this week, the department reports that from June 24, 2022 — the day of the Dobbs decision — through early June 2023, a total of 925 abortions were completed in Vermont. Of those, 154 were performed on non-Vermont residents — roughly 17%. (Due to reporting lag time, the department was unable to provide data from the latter portion of June 2023.)
By comparison, in all of 2021, 215 out-of-state patients obtained abortions in Vermont, representing nearly 21% of the 1,033 abortions completed in the state that year.
Since 2018, the proportion of out-of-state patients who obtain abortions in Vermont has remained relatively stable, hovering between 17 and 22% every year. But mirroring national trends, the total number of abortion patients in the state — both those who hail from Vermont and those who don’t — has trended downward.
In the year since Roe fell, a handful of patients traveled to Vermont from far-flung states where an abortion is difficult to obtain: Alabama, Louisiana, Tennessee and Texas, to name a few. But most out-of-state patients traveled from nearby states, where access to abortion is, in theory, about on par with Vermont: Connecticut, Maine, Massachusetts, New Hampshire, New York and Rhode Island. More than half of all out-of-state patients came from New Hampshire, mirroring past years’ trends.
Vermont’s clinics had anticipated such a trend, according to Lucy Leriche, vice president of Vermont public affairs for Planned Parenthood of Northern New England. “There are a lot of reasons why people from out-of-state are getting an abortion in our region,” she said, speaking of Vermont as well as New Hampshire and Maine.
Sometimes northern New England is where the patient has a family member or support system to assist in the process, Leriche said. Perhaps they are fleeing a domestic violence situation. They could be attending college here, but a legal resident elsewhere. Maybe they just want more privacy. Or perhaps, if they hail from a nearby state that has more patients, such as New York or Massachusetts, they couldn’t get an appointment at home. A domino effect in appointment availability can ensue, Leriche said.
Planned Parenthood — the largest provider of abortions in Vermont, and nationwide — declined to provide state-specific data on its own out-of-state patients, citing concerns over patient privacy and safety. But in Maine, New Hampshire and Vermont combined, the organization earlier this month reported a 12.5% increase in out-of-state patients “seeking abortion at our health centers,” according to a June press release.
Beyond patient data, Leriche said the impact of the Dobbs decision was palpable in other ways. Planned Parenthood of Northern New England’s call center was “inundated” immediately after the ruling was made, she said. Online, the organization’s website had its largest one-day spike in web traffic on June 24, 2022, the day of the court’s ruling. “That is, I think, a really strong indicator of the response,” Leriche said.
The Dobbs decision “is very destabilizing and very anxiety-producing, and causes a lot of confusion and anxiety and fear and panic,” Leriche said.
Leriche said the organization is trying to keep its messaging on target, emphasizing that abortion remains legal in Vermont. This legislative session, state lawmakers passed landmark shield laws protecting Vermont-based abortion providers — and to some extent, patients who travel to the state — from out-of-state abortion prosecutions or investigations.
NC’s new abortion restrictions take effect tomorrow. Here’s what to expect.
By Rachel Crumpler
Beverly Gray, an OB-GYN at Duke Health who provides abortion care, expects that turning away people seeking abortions in North Carolina will be a daily occurrence beginning tomorrow, when the state’s new restrictions passed by Republican lawmakers take effect.
Overnight, abortion access will significantly diminish as the time frame for seeking most abortions in the state drops from 20 weeks of pregnancy to 12 weeks.
Gray said cutting weeks of access in the state will make turning patients away from care — which already happened under the 20-week ban — more frequent.
That’s devastating to her, to her colleagues and to many women, she said.
“I think about when we turn someone away, will they be able to make it to another state?” Gray asked. “And if they can’t, what is their life going to be like? What is their child’s life going to be like?”
It’s not lost on Gray why she will be turning more people away — timelines set by North Carolina lawmakers over the objections of medical professionals and a veto by Gov. Roy Cooper. Gray still has the same skills to help patients in an array of situations, but her hands will be newly tied — taking previously available options for reproductive health care off the table.
Amy Bryant, another OB-GYN and abortion provider, knows the new North Carolina law will put care out of reach for many patients, such as a 17-year-old whom she treated a few weeks ago. The teen, who was just finishing high school, sought an abortion when she was 13 weeks and one day pregnant. Tomorrow, that patient would be left to carry the pregnancy to term or travel out of state.
“That’s just going to happen so much more,” Bryant said. “It’s just unfair.”
While most abortions occur before 12 weeks, Bryant said, there are plenty of scenarios when that’s not possible. At least 1,878 North Carolinians obtained abortions after 12 weeks of pregnancy in 2021 out of a total 27,305 who had abortions, according to the latest data available from the state health department.
North Carolina’s new law does provide some exceptions — for rape, incest, fetal anomalies and risk to the mother — that allow an abortion after 12 weeks. Still, Bryant said, some of the most vulnerable patients will be outside the window of care, such as teenagers with irregular periods who often identify pregnancy later, or those who need more time to pull resources together.
Gray has similar concerns about access to care.
“There are a lot of complex social reasons that impact why people need care,” Gray said. “I think a lot of those patients don’t fall into the exceptions — patients who may be living in poverty, who are working multiple jobs, who already have kids, who have delays in care because they at baseline don’t have access to health care.”
“My colleagues and I want to abide by the laws, and we want to provide the best possible care,” Bryant said. “There are times where that really does come into conflict, and it’s gotten worse.”
New era of care
Since the Supreme Court’s Dobbs decision in June 2022 handed the authority to regulate abortion back to states and their elected officials, North Carolina providers working in reproductive health care have faced a challenging year navigating the shifting legal landscape. Tomorrow, they will enter a new era, adjusting their practices to conform to the added constraints on their work.
In addition to cutting by eight weeks the time window allowed for most abortions, lawmakers placed more requirements on women seeking abortions and on their providers.
One of the biggest changes is requiring an in-person appointment for state-mandated counseling at least 72 hours before an abortion. Previously, this pre-procedure counseling could occur over the phone or online. Gray said for patients and providers, this will be one of the most difficult requirements to adjust to and, she emphasized, it’s not medically necessary.
As a result, patients will be required to visit clinics at least twice — many needing to travel long distances to reach one of the state’s 14 abortion clinics spread over nine counties. The additional appointment will necessitate extra time off work, miles driven, hotel stays and child care costs.
“We expect that to be a significant barrier for many patients, and probably an insurmountable one,” Molly Rivera, Planned Parenthood South Atlantic spokesperson, told NC Health News in May. “Especially for folks in rural parts of the state who have to already drive hours to get to an abortion clinic. Especially for folks that don't have paid time off of work. Especially for people who already have kids at home.”
For providers and clinics, adding an extra appointment to an already busy workload will create another layer of complexity to scheduling. There also are new reporting requirements that physicians say will be burdensome.
“I would rather spend that time with my patient and their family,” said Caledonia Buckheit, an OB-GYN in the Triangle. “I don't want my time and effort to be towards paperwork and legal — these things that are not patient-centered.”
Several other provisions in Senate Bill 20 are being challenged by Planned Parenthood South Atlantic and Gray in a lawsuit that was filed June 16 in U.S. District Court. The health care providers argue that specific provisions are so vague or contradictory that doctors are uncertain about what’s lawful.
After the lawsuit was filed, lawmakers at the General Assembly revised several of the challenged abortion provisions this week by passing amendments to a separate bill. For example, one revision clarified that medication abortions are permitted up to 12 weeks in the state. Previously, language in Senate Bill 20 stated in one place that the age of the fetus could be “no more than 70 days,” or 10 weeks.
Gov. Cooper signed the revised provisions into law Thursday afternoon, less than 48 hours before the new restrictions take effect.
"In addition to being dangerous for women, the rushed abortion ban was so poorly written that it is causing real uncertainty for doctors and other health care providers,” Cooper wrote in a statement about signing House Bill 190. “This bill is important to clarify the rules and provide some certainty, however we will continue fighting on all fronts the Republican assault on women’s reproductive freedom."
At a federal court hearing for the lawsuit heard in Greensboro on Wednesday, the plaintiffs and defendants agreed that the new language resolves issues with several provisions. However, the passage does not resolve the entirety of the lawsuit. The remaining differences likely will be addressed through future legal proceedings.
“Our lawsuit was never going to be able to give North Carolinians the bodily autonomy that they deserve,” Rivera said after the court hearing. “This law passed. It's happening. But we did come to the court to get clarity so that we know how to comply with this sweeping law so that we can help patients navigate this reality.”
Other portions of the bill, such as the mandate that any abortion after 12 weeks be provided in a hospital and the implementation of any new, potentially stringent licensing rules on the state’s abortion clinics, will not go into effect until October.
How sick is sick enough?
The new law about abortion does provide some exceptions for rape, incest, fetal anomalies and risk to the mother that allow abortions later in pregnancy, but physicians have concerns about how workable those are in practice.
Lisa Carroll, a high-risk pregnancy OB-GYN worries about her patients — many of whom have chronic illnesses that are exacerbated by pregnancy. Many conditions are not immediately life-threatening, but pregnancy could cause long-term health risks.
For example, Carroll recently treated a pregnant patient with kidney disease. Carrying the pregnancy caused significant dysfunction to the woman’s kidneys, for which she required dialysis. Carroll had a long conversation about her options to continue the pregnancy or terminate. The patient chose to continue the pregnancy, but Carroll said she’s unsure if the same situation presented next week would be considered life-threatening enough to meet the law’s exception.
‘Particular wording’
Carroll spends most of her time screening for and diagnosing fetal anomalies in pregnancies, and the law allows abortions up to 24 weeks in cases where a “life-limiting” anomaly is found.
Medical professionals have voiced concern over the phrase “life-limiting” anomaly, calling it broad and open to interpretation.
“What is life-limiting?” Carroll asked. “Does that mean that the fetus isn't expected to live a month after birth? Isn't expected to live a year after birth? Isn't expected to live to the age of 10?”
Rachel Veazey, a reproductive genetic counselor in the Triangle, agrees that “life-limiting” is ambiguous.
“It’s really particular wording that, I think, is going to throw our field for a loop,” Veazey said.
Veazey explained that very few conditions are considered definitively lethal — or always causing a newborn baby to die. Many fetal anomalies are a spectrum that often catch expecting parents by surprise. Often, she said, they result in a child with such profound disabilities that their quality of life is severely diminished.
“With a lot of families, we end up having conversations about quality of life versus life-limiting,” Veazey said. “There's a lot of anomalies or genetic conditions that very much alter the picture of what families imagine when they enter into a pregnancy that is not compatible with their life, and they would view it as life-limiting. But we know that's not what the rough definition of what the law is going for.”
‘Counseling conundrum’
In some ways, though, Carroll said not having a definitive list of conditions is helpful because individual physicians and health care institutions can determine what they are comfortable deeming life-limiting based on the context of each individual case.
Operating in this gray area is also problematic, she said.
“It is good to allow for physician judgment, but the problem is that physician judgment is now open to criminalization,” Carroll said. “If there are other physicians who disagree, or who say that it's not life-limiting, or it's not life-limiting in all cases, or wasn't life-limiting in that particular case — then I may be criminalized for that individual judgment.
“That is not something that is normal or appropriate or fair in the practice of medicine, and it may lead physicians to be counseling patients based not on the patient's best interest or the fetus’ best interest.”
Veazey said the patients she counsels with identified fetal anomalies regularly choose to terminate the pregnancy. While she expects a good portion of fetal anomalies to be detected by 24 weeks, it will not encompass all conditions, nor necessarily account for those who are delayed starting prenatal care or who face delays due to the state’s new abortion restrictions. That’s why she believes her job may become more focused on grief counseling in the months ahead as she sees more patients who may be carrying pregnancies to term who would have — in a different legal landscape — opted for abortion.
“A lot of the conversations we have with families that are continuing with pregnancy are helping them understand what the health care management looks like for that child or individual with a birth defect or genetic condition,” Veazey said. “Imagining doing that with or for someone who wouldn't have on their own volition decided to continue a pregnancy is a different kind of counseling.”
Although medical professionals see potential ambiguity with other conditions, the law does make one thing clear in regard to fetal anomalies: New language bans abortions at any gestational age due to the identification of the fetal abnormality of trisomy 21, known as Down syndrome — one of the most common genetic differences in a human embryo.
“It's going to create a very strange counseling conundrum for high-risk OB doctors, for all general providers, anybody who provides prenatal care,” Carroll said.
Loss of options
Tomorrow North Carolina will join the ranks of about 20 other states across the country that have banned or increasingly restricted abortion access since Dobbs. Before this legal change, the state served as one of the last remaining abortion access points in the South.
In states with new restrictions, there were fewer abortions, while the numbers show that many women traveled to other states for procedures. In sum, though, the Society for Family Planning has collected data on abortions across the country and found that in the first nine months after the Supreme Court overturned Roe, there were a cumulative 25,640 fewer abortions in the U.S.
“We know that bans or restrictions on abortion care don't stop abortions from happening,” Rivera from Planned Parenthood South Atlantic said. “They just make it harder for people to do it, which inevitably pushes them further into their pregnancy.
“So even a patient who has decided long ago that not only did they realize they were pregnant but they decided they didn't want to be, they are not able to get an abortion right away. They first have to figure out whether or not they can get it in their home state. And if they learn that they cannot, they have to figure out where to get it next. And that's complicated.”
Gray wishes that lawmakers would trust women to make their own reproductive health decisions.
“Patients are really the experts of their lives, and they know what they're able to handle and not able to handle,” Gray said. “I think they make really thoughtful decisions, and this law makes it harder for them to be thoughtful. It makes it harder for us to provide evidence-based care and just creates chaos for an already busy and taxed medical system. It doesn't improve care.”
Tell us your story about abortion access
NC Health News will be continuing to cover the effects of increased abortion restrictions in the months ahead and the best way for us to do that is with your help — hearing concrete examples of how you are navigating the new law. Have you been affected by new abortion restrictions as a medical professional or a patient? NC Health News is interested in hearing your experience.
After the fall of Roe, physicians confronted their toughest year working in reproductive health care
By Rachel Crumpler
After graduating from a medical school in the Northeast, Caledonia Buckheit came south to Duke University Hospital to complete her obstetrics and gynecology residency. She finished up last June and found work in North Carolina — ready to provide comprehensive reproductive health care to patients, including abortion.
Just weeks after finishing, the Supreme Court overturned Roe v. Wade. The June 24 decision in Dobbs v. Jackson Women’s Health Organization eliminated the constitutional right to abortion that had existed for nearly half a century.
“Controlling women’s bodies has always been a topic but I didn’t really think it would get to this,” Buckheit said.
Suddenly, working in reproductive health care got a lot more complicated.
On top of the challenges that come with entering a new profession, Buckheit — like everyone else working in reproductive health care — has spent the past year navigating a shifting legal landscape and all the questions and unknowns that come with continuing to provide care.
“It’s just been really disheartening, feeling like my patients have less autonomy,” said Buckheit, a general OB-GYN working at a private practice in the Triangle.
Rep. Sarah Stevens takes questions during an evening press conference with reporters on the Republicans’ proposed 12-week abortion restrictions on May 2. With Stevens were a group of women Republicans who had been part of a group that hashed out the proposal. (R to L) Rep. Kristin Baker (R-Concord), Rep. Jennifer Balkcom (R-Hendersonville), Rep. Donna White (R-Clayton), Sen. Lisa Barnes (R-Spring Hope), Sen. Amy Galey (R-Burlington), Rep. Diane Wheatley (R-Fayetteville), Rep. Erin Paré (R-Holly Springs), Sen. Vickie Sawyer (R-Mooresville) and Sen. Joyce Krawiec (R-Winston-Salem). Credit: Rose Hoban
Jenna Beckham, an obstetrician-gynecologist from Wake County, speaks against Senate Bill 20 during a committee meeting at the General Assembly on May 3. “The requirements proposed in this bill are not evidence-based or in any way beneficial to patients, but rather create further barriers and hoops for patients and providers alike to have to jump through,” she told lawmakers. Credit: screenshot from NC General Assembly Youtube feed
On short notice, hundreds of abortion rights advocates showed up in force at the state capitol on May 3. They filled Bicentennial Plaza, across from the legislative building, to participate in an afternoon rally organized by Planned Parenthood South Atlantic. Credit: Rachel Crumpler
Planned Parenthood South Atlantic President and CEO Jenny Black spoke against Senate Bill 20 during a rally on Bicentennial Mall, across from the legislative building on May 3. “This is the moment we’ve been preparing for since the Supreme Court overturned Roe v. Wade and gave state legislators the power over our bodies in our health care decisions, but I want to be real with y’all,” Black told the crowd. “This is much worse than we feared. This is no compromise. This bill is a monster abortion ban.” Credit: Rachel Crumpler
Democratic House Minority Leader Robert Reives speaks at the end of the debate over the new abortion restrictions on May 3. “To say that this was a compromise bill is a misnomer,” Reives said. “A compromise bill is people with completely opposing views sitting in a room and coming out with a decision that everybody even though not happy with can live with.” Credit: Rachel Crumpler
Protesters at a rally held on May 13 where Gov. Roy Cooper vetoed SB 20, a bill passed by the General Assembly that limits most abortions after 12 weeks and creates other requirements for women and their providers to fulfill in order for the procedure to take place. Credit: Rose Hoban
Gov. Roy Cooper holds up the veto stamp after he applied it to his veto of SB 20 during a rally held on May 13. “This bad bill needs a return to sender,” Cooper told the crowd as they erupted into applause and chants of “Veto! Veto! Veto!” Credit: Rose Hoban
People on both sides of the abortion debate showed up at the General Assembly building on May 16 to encourage lawmakers to vote their way on the veto override of Senate Bill 20. Credit: Rose Hoban
Supporters of abortion rights sat in the gallery above the House of Representatives on May 16, waving their hands when agreeing with speakers and giving the thumbs down when in opposition. Credit: Rose Hoban
Charlotte Rep. Tricia Cotham, whose defection from the Democrats to the Republican Party sealed a supermajority in the House of Representatives, made her way to the office of Speaker Tim Moore (R-Kings Mountain) after the override vote was completed in the House. Credit: Rose Hoban
After the Senate voted to override Gov. Cooper’s veto, several Democratic senators, including (L to R in foreground) Sydney Batch (Raleigh), DeAndrea Salvador (Charlotte), Gale Adcock (Cary), Natasha Marcus (Davidson), Michael Garrett (Greensboro) and Gladys Robinson (Greensboro), promptly stood and held signs reading, “Politicians make crappy doctors.” Credit: Rachel Crumpler
Cora Field and Loretta Pfeiffer, both 16, pose with their pro-choice signs following the Senate vote overriding Cooper’s veto on May 16. They said they cried when lawmakers overrode Cooper’s veto. “I’m witnessing a really sad day in history,” Pfeiffer said. “I feel like my rights are being taken away and I can’t do anything about it.” Credit: Rachel Crumpler
Adjusting practice
Even for those who have been practicing for years, like OB-GYN Amy Bryant, it’s unquestionable that the past year has been the most challenging and exhausting time to be in the reproductive health care field.
Since the fall of Roe, the legal landscape has been continuously shifting. Abortion providers across the nation and in North Carolina have had to adjust their practices to stay within the bounds of the law.
“When I think back to the early days after the Dobbs decision after Roe v. Wade was overturned, I just really think about the chaos and the uncertainty and the difficulties that we confronted, like, almost instantaneously with this new law of the land,” Bryant said. “It was truly just kind of scary.”
Beverly Gray, another long-time OB-GYN who works with many high-risk and complicated pregnancies, said she was startled by how quickly some neighboring states took action to cut access to abortion. For months, North Carolina — and its 14 abortion clinics located in nine counties — became a critical abortion access point in the Southeast, providing care to an increased number of out-of-state patients.
Over the past year, the legal landscape for abortion access has changed in North Carolina. Credit: Rachel Crumpler/NC Health News
In August, North Carolina physicians had to adjust their practices for the first time following the Dobbs decision when a federal judge reinstated North Carolina’s 20-week abortion ban, citing the disappearance of constitutional protections on the procedure. The ruling cut the window of time pregnant people had for seeking abortions in the state from fetal viability, which typically falls between 24 and 26 weeks of pregnancy.
The loss of those weeks was palpable for abortion providers like Gray who had to turn patients beyond 20 weeks away — patients she could previously care for. In her practice, she said those patients mainly consisted of people who received a diagnosis of severe birth defects.
“We didn’t know when the law might change and how we were going to respond if somebody was already scheduled and ready to go and they’d come from eight hours away,” Bryant said. “We didn’t know if we would still be able to care for them or not. That was just not a good way to practice medicine.”
Next month, once again, a change in law will necessitate people who work in reproductive health care to alter their practices to conform to new constraints on their work.
Even a month after Senate Bill 20 was passed and the veto overridden, there are still more changes, as just this past week, the state Senate added an amendment to a separate bill that clarifies some of the timing of restrictions.
Gray said it’s not normal for physicians to have to significantly rethink how they practice, especially so many times over the span of one year. She emphasized that practice changes are being dictated by an arbitrary change in law, not as a result of improved medical guidelines.
“It’s completely disruptive to our practice, to our lives, to our day-to-day,” Gray said.
It’s a heavy load to carry — added stresses and tasks that Gray said most other physicians don’t have to experience.
“It’s really just exhausting on so many levels because I’m doing all that and at the same time still providing care, still doing all the other work that’s required as a physician and now it’s just all these extra layers,” Gray said.
When Gray decided to go to medical school, she never thought her role as an OB-GYN would involve so much advocacy and parsing new laws, but that’s what it’s turned into in the post-Dobbs period.
Bryant agrees that the role has changed significantly over the past year.
“I have spent so much time poring over the legal issues related to my work,” she said. “It is not what I would like to be doing.
“I think that pregnancy is just far too complicated to be legislated. And when nonmedical professionals start to try to legislate it, it becomes even more complicated to really understand the nuance — to be able to address the nuances in the individual situations that arise when a person becomes pregnant. This is not in any way what I expected my life to become.”
Buckheit, the new OB-GYN, didn’t expect lawmakers would be dictating how she can do her job, either. And she believes they may have written the law differently if they interacted with pregnant patients on a daily basis.
“I truly feel that if lawmakers spent a week at Planned Parenthood or spent a week in a high-risk OB-GYN office, they would have a really different take,” Buckheit said. “There’s so much complexity and nuance to what we see and what patients and families are going through.”
For example, she’s had to read the state-mandated counseling script 72 hours before an abortion to patients whose babies have serious fetal anomalies.
“It’s like, adoption is an option, parenting is an option,” Buckheit said. “I’m saying this to someone whose baby doesn’t have a brain. It’s just so cruel.”
The work, particularly in an environment of tightening restrictions, also takes an emotional toll.
“Living in this world now where basic health protections are no longer in place is very difficult,” Bryant said. “Obviously, for patients and also for providers who experience a whole lot of moral distress, knowing that you can care for someone yet not be able to because lawyers, legislators, the courts are telling you that you can’t. It’s a really uncomfortable and distressing place to be.”
Gray and Bryant can’t help but think about the patients they’ve cared for recently and consider whether the same options will be available after July 1.
It’s a devastating reality, Gray said, to know she still has the same skills to help patients in an array of situations but her hands will soon be tied by new rules where she will have to turn some people away she could previously care for.
“I think every single patient that we’re able to care for is meaningful and important, and we’re able to help change the trajectory of people’s lives,” Gray said. “I worry about all of those people that didn’t make the exceptions [to the new rules], but still have really important things that are happening in their lives and the lack of compassion for the people that didn’t make these arbitrary exceptions. It’s heartbreaking.”
Despite the more burdensome and taxing legal landscape, those providing reproductive health care remain committed to providing as much access as possible. The patients are the motivation.
“I feel this immense responsibility to get it right and to still be able to provide care for people,” Gray said. “There’s a huge stress and responsibility.”
Tell us your story about abortion access
NC Health News will be continuing to cover the effects of increased abortion restrictions in the months ahead and the best way for us to do that is with your help — hearing concrete examples of how you are navigating the new law. Have you been affected by new abortion restrictions as a medical professional or a patient? NC Health News is interested in hearing your experience.
One year after the fall of Roe v. Wade, abortion care has become a patchwork of confusing state laws that deepen existing inequalities
Poll: Mississippi Republican voters cool on abortion ban
Mississippi politicians have long viewed being anti-abortion as a key to winning elections, working diligently for years to stretch the limits of the law and pass some of the nation’s most restrictive bans.
But based on a new Mississippi Today/Siena College poll, being anti-abortion may not be the key electoral issue that politicians – especially Republican politicians – have believed it to be.
A poll of Mississippians who say they will vote in the Aug. 8 Republican primary found that 45% support repealing the state’s “trigger law” that bans most abortions in the state. Another 44% of likely Republican voters oppose repealing the ban, and 11% said they were not sure.
Editor’s note: Poll methodology and crosstabs can be found at the bottom of this story. Click here to read more about our partnership with Siena College Research Institute.
Mississippi’s trigger law went into effect in 2022, when the U.S. Supreme Court overturned Roe vs. Wade. That decision effectively meant that abortion was no longer a national right and that the issue could be decided by each state.
It was a Mississippi case that led to the overturning of Roe. After the Supreme Court decision, the Republican leadership of the state proudly proclaimed Mississippi to be solidly pro-life, with some saying it was the nation’s “safest state for the unborn.”
The poll results are especially notable since the respondents are those who say they intend to vote in Republican primary in August. Generally speaking, it is believed that Republican primary voters tend to be staunchly anti-abortion while Democratic voters support abortion rights.
But based on the new poll, abortion might not be any longer the hot-button social issue that Republicans use to attack Mississippi Democrats and link them to national Democrats.
That issue, according to the results of the poll, could become rights of transgender Americans. According to the poll, likely Republican primary voters by an overwhelming 70%-to-19% margin oppose “repealing the current ban on gender affirming healthcare for any trans person under 18 years of age.” The remaining 11% of the poll respondents were undecided.
Earlier this year during the 2023 legislative session, Republican leaders pushed through a bill banning gender affirming care for minors. The bill prohibits medical providers in Mississippi from providing the care and also appears to ban parents from seeking out-of-state care for their children, though it is unclear how that provision would be enforced.
In the 2023 session, Republican legislative leadership also attempted to take steps to ensure that laws in the state banning most abortions are not weakened.
The Legislature made an unsuccessful effort to revise the state’s ballot initiative process that was struck down in 2021 on a technicality by the state Supreme Court. The initiative process allows voters to gather signatures to bypass the Legislature and place issues on the ballot. The House leadership, led by Speaker Philip Gunn, wanted the new initiative process to ban efforts of placing abortion issues on the ballot. The Legislature ultimately was unable to pass a law restoring the initiative.
Of course, the one time that Mississippians voted on the issue of abortion under the old and now invalid initiative, they rejected the so-called “personhood amendment” by a 58% to 42% margin. The personhood proposal on the ballot in 2011 defined a person “to include every human being from the moment of fertilization, cloning or the equivalent thereof.” Then-Lt. Gov. Phil Bryant said at the time a vote against personhood would be “a victory for Satan.”
Since the U.S. Supreme Court overturned the national right to an abortion in 2022, six states have voted on abortion. In all of those states, the electorate voted — usually by large margins — to expand abortion rights. Some of those states, such as Kansas, Kentucky and Montana, are seen as conservative as Mississippi.
On other issues, likely Republican Party primary voters, according to the poll:
Support eliminating the grocery tax 76% to 15%, with 9% undecided or not answering.
Support eliminating the state personal income tax 71% to 18%, with 11% not sure.
Support full funding of public education through the Mississippi Adequate Education Program 57% to 16%, with 26% having no opinion or not knowing.
Support expanding Medicaid 52% to 35%, with 13% not sure.
The Mississippi Today/Siena College Research Institute poll of 646 registered voters was conducted June 4-7, 2023, and has an overall margin of error of +/- 4.8 percentage points. Siena has an ‘A’ rating in FiveThirtyEight’s analysis of pollsters.